
Arthrology and Infections — MCQs

On this page
Most common cause of AVN of the hip is -
For a distended knee joint, which of the following positions is most comfortable?
Choose the wrong statement regarding chondromalacia patella _____:
A 10-year-old child with known hemophilia presents with ankle pain. X-ray shows a lytic lesion with sclerotic rim at the calcaneum. What is the most likely diagnosis?
12 years male came with swelling of lower end tibia which is surrounded by rim of reactive bone. What is most likely diagnosis?
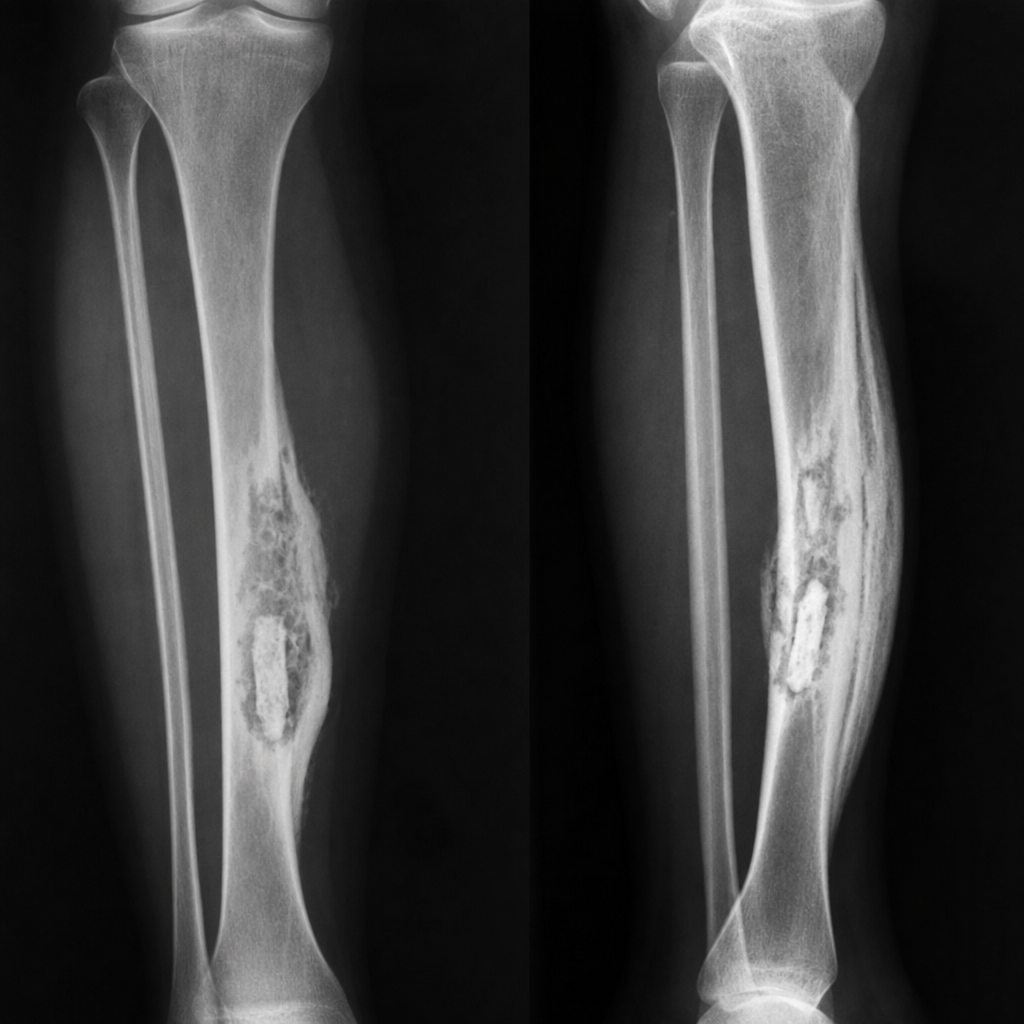
A patient had osteomyelitis in their left tibia 2 years ago. They now present with pain and swelling at the same site. X-ray shows bone destruction, sequestrum, and involucrum. What is the most likely diagnosis?
A 25-year-old male presents with chronic leg pain and a draining sinus. What is the most likely diagnosis?
A 10-year-old boy presents with swelling of the knee and fever. Blood tests reveal elevated ESR and CRP. An X-ray of the knee shows periosteal elevation. What is the most likely diagnosis?
What clinical finding is critical for identifying chronic osteomyelitis after sequestrectomy?
What is the most appropriate treatment for a patient with a suspected Brodie's abscess?
Practice by Chapter
Septic Arthritis
Practice Questions
Osteomyelitis
Practice Questions
Tuberculosis of Bones and Joints
Practice Questions
Fungal and Parasitic Infections
Practice Questions
Diabetic Foot Infections
Practice Questions
Prosthetic Joint Infections
Practice Questions
Reactive Arthritis
Practice Questions
Management of Joint Infections
Practice Questions
Prevention of Orthopaedic Infections
Practice Questions
Biofilms in Orthopaedic Infections
Practice Questions
Antibiotic Prophylaxis
Practice Questions
Implant-Related Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app