
Arthrology and Infections — MCQs

On this page
With reference to frozen shoulder, consider the following statements: 1. It is associated with diabetes and heart disease. 2. It may follow minor trauma. 3. Its differential diagnosis are infection and fractures. 4. Treatment of choice is surgery. Which of the statements given above are correct?
A 18-year-old boy presents with tenderness, warmth over the bone, and fever. His ESR and CRP are elevated, and blood cultures were previously positive. The radiograph is shown below. What is the most likely diagnosis?
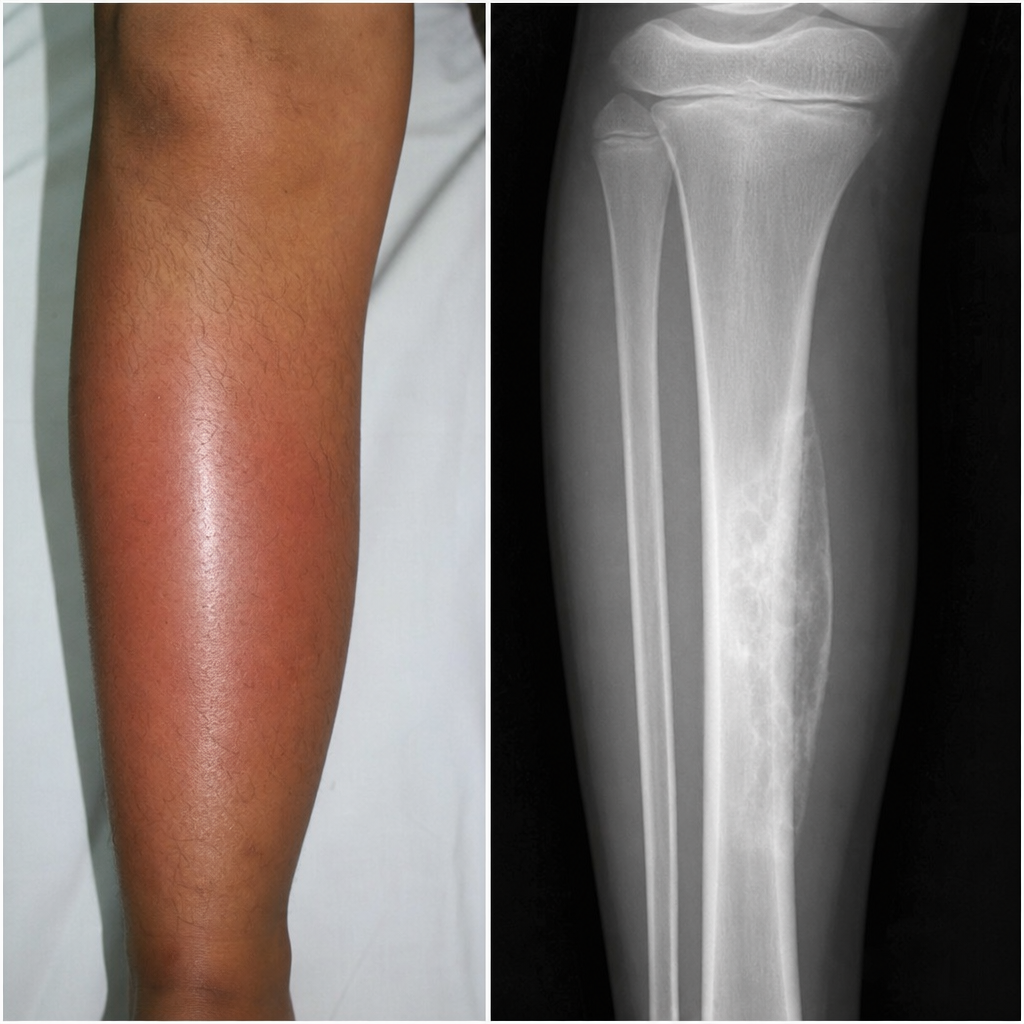
An 18-year-old boy presents with a several-week history of tenderness, warmth over the bone, and low-grade fever, elevated ESR and CRP levels. The radiograph is shown below. What is the most likely diagnosis?
Which of the following statements about tubercular osteomyelitis is NOT true?
Tom-smith arthritis results from
Which of the following is/are established risk factor(s) for osteonecrosis of the femoral head?
Charcot's/neuropathic joint are most commonly seen in
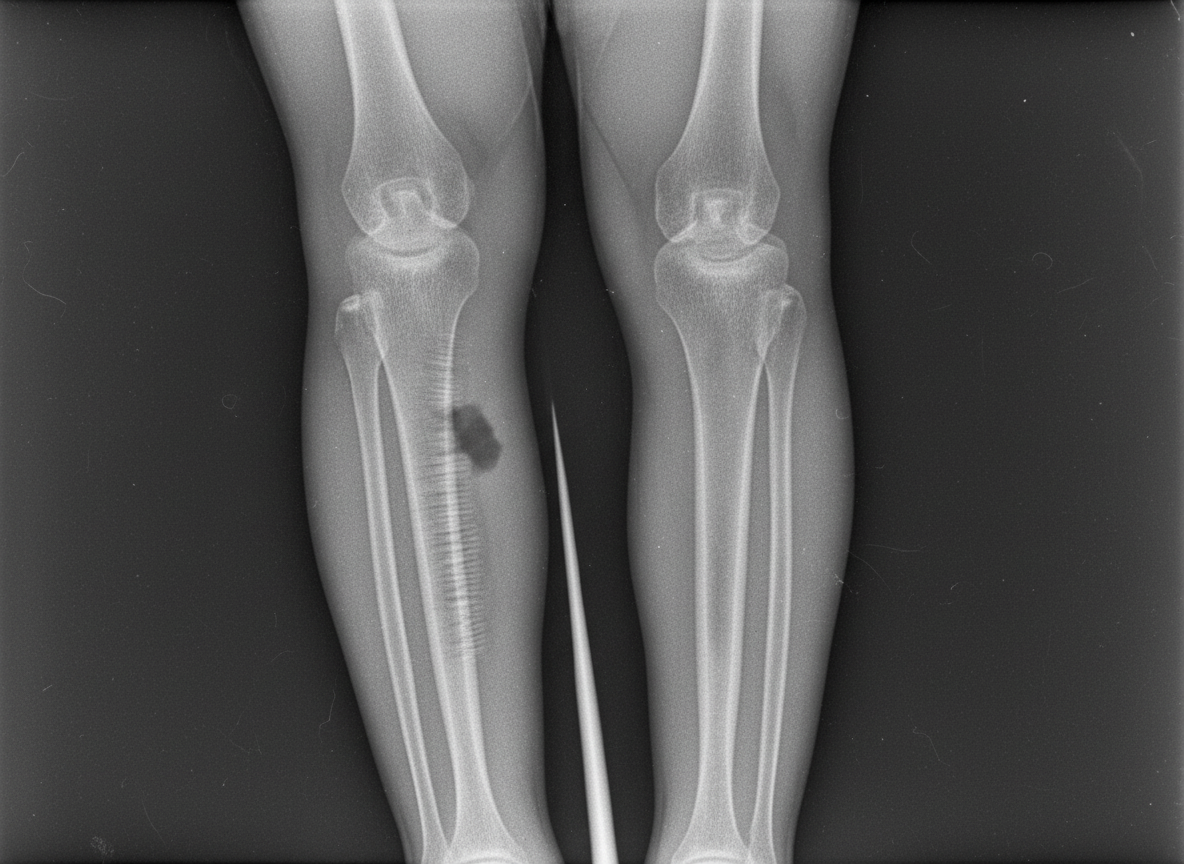
A patient has a history of pain and swelling at the same site for 2 years. An X-ray shows the following features. What is the most likely diagnosis?

All of the following are associated with frozen shoulder except
A 60-year-old man with diabetes mellitus presents with a painless, swollen right ankle joint. Radiographs of the ankle show a destroyed joint with a large number of loose bodies. The most probable diagnosis is:
Practice by Chapter
Septic Arthritis
Practice Questions
Osteomyelitis
Practice Questions
Tuberculosis of Bones and Joints
Practice Questions
Fungal and Parasitic Infections
Practice Questions
Diabetic Foot Infections
Practice Questions
Prosthetic Joint Infections
Practice Questions
Reactive Arthritis
Practice Questions
Management of Joint Infections
Practice Questions
Prevention of Orthopaedic Infections
Practice Questions
Biofilms in Orthopaedic Infections
Practice Questions
Antibiotic Prophylaxis
Practice Questions
Implant-Related Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app