
Arthrology and Infections — MCQs

On this page
A Baker's cyst is a type of:
A child presents with subacute localized pain and low-grade fever. Imaging reveals a well-circumscribed ring-shaped lytic lesion with a thick sclerotic rim in the metaphysis of the tibia, with no nocturnal pain pattern. Which of the following is the most likely diagnosis?
A 42-year-old woman laborer presented with visible, soft, and fluctuating swelling in front of the knee, over the patella and some discomfort or difficulty with knee movement, MRI findings are given below. What is the diagnosis?
A 15-day-old neonate was brought with complaints of high grade fever for 2 days and decreased playing movements of right leg. On examination the right knee joint is red, tender and shows fluctuation. All are true about the condition shown except:

All the following statements regarding this image are true except: (Recent NEET Pattern 2016-17)

All are correct about the X-ray film shown below (antibiotic PMMA beads) except:

Which form or manifestation of osteomyelitis is shown below?

In the given image of chronic osteomyelitis choose the correct sequence:
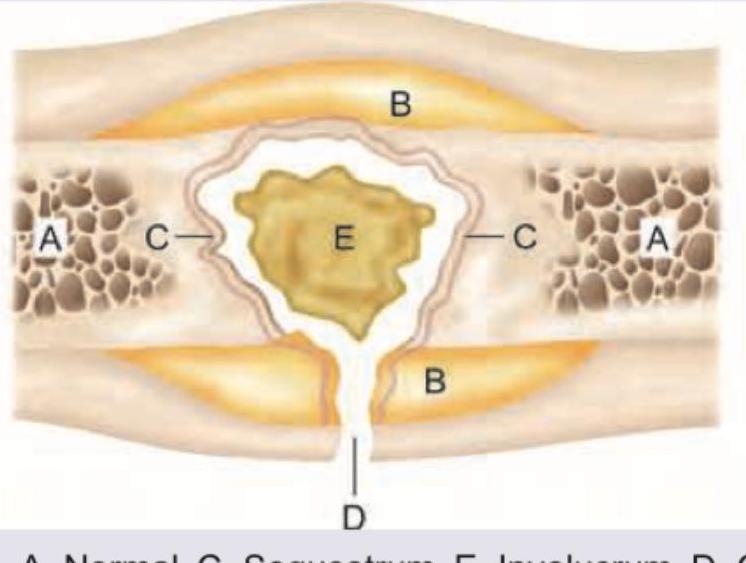
A 10-year-old child presents with fever and wound with discharging pus from right thigh for 4 months. Given below is the X -ray of the patient. Identify the marked area:

A 52-year-old female complains of increasing pain in the right shoulder. She is also finding it increasingly difficult to do overhead abduction of the affected joint. She had been diagnosed as a diabetic 20 years back and is on treatment since then. What is the most likely cause of her clinical condition?
Practice by Chapter
Septic Arthritis
Practice Questions
Osteomyelitis
Practice Questions
Tuberculosis of Bones and Joints
Practice Questions
Fungal and Parasitic Infections
Practice Questions
Diabetic Foot Infections
Practice Questions
Prosthetic Joint Infections
Practice Questions
Reactive Arthritis
Practice Questions
Management of Joint Infections
Practice Questions
Prevention of Orthopaedic Infections
Practice Questions
Biofilms in Orthopaedic Infections
Practice Questions
Antibiotic Prophylaxis
Practice Questions
Implant-Related Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app