
Arthrology and Infections — MCQs

On this page
Genu valgum deformity is seen in all except?
What is the commonest site for osteochondritis dissecans in the elbow?
The Thomas test helps to detect which of the following conditions?
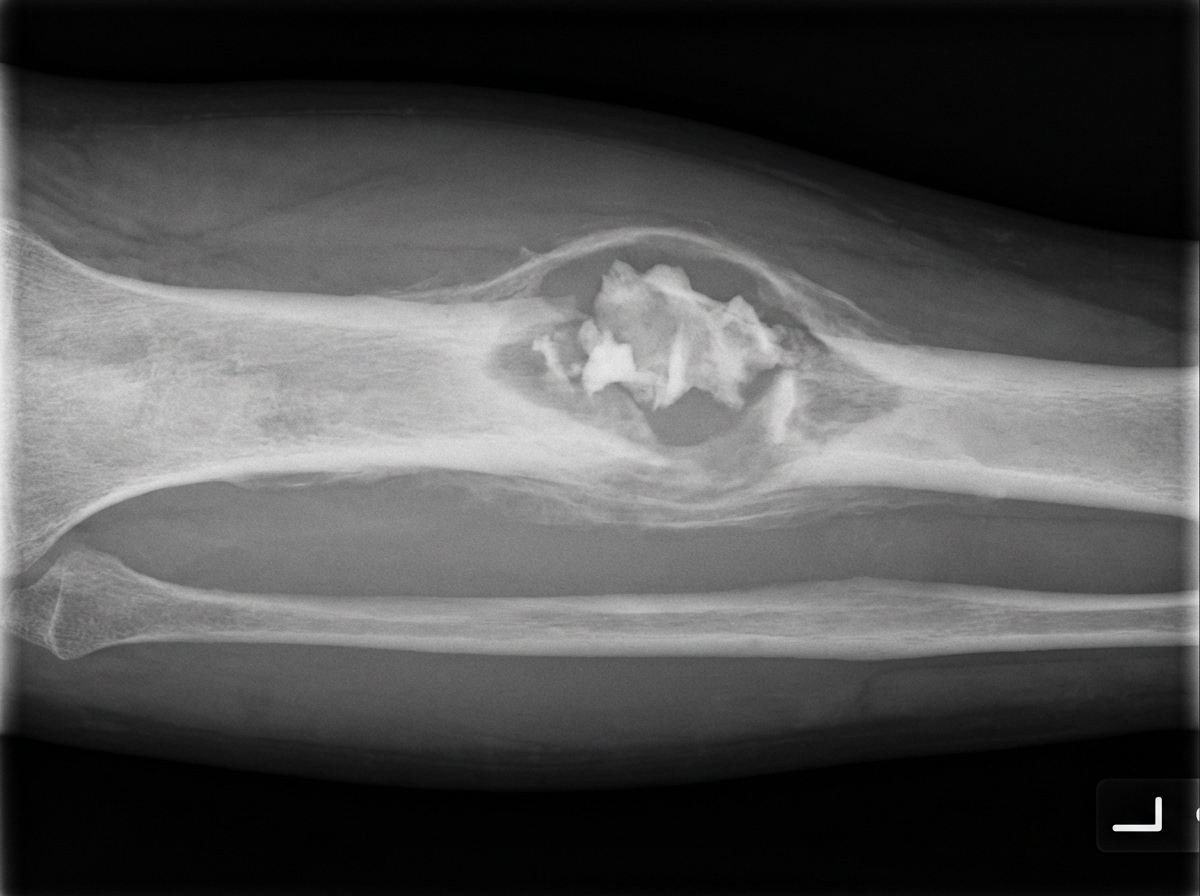
A patient has a history of similar complaints 2 years back at the same site, and now presents with pain and swelling. X-ray shows certain features. What is the most likely diagnosis?
Joint mice are seen in which of the following diseases?
What is spina ventosa?
What is the gold standard diagnostic method for guiding antibiotic therapy in a case of osteomyelitis?
Baker's cyst is a swelling which occurs in:
Septic arthritis most commonly affects which joint in infants?
What is the most common type of patellar bursitis?
Practice by Chapter
Septic Arthritis
Practice Questions
Osteomyelitis
Practice Questions
Tuberculosis of Bones and Joints
Practice Questions
Fungal and Parasitic Infections
Practice Questions
Diabetic Foot Infections
Practice Questions
Prosthetic Joint Infections
Practice Questions
Reactive Arthritis
Practice Questions
Management of Joint Infections
Practice Questions
Prevention of Orthopaedic Infections
Practice Questions
Biofilms in Orthopaedic Infections
Practice Questions
Antibiotic Prophylaxis
Practice Questions
Implant-Related Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app