
Arthrology and Infections — MCQs

On this page
Which of the following conditions can cause bony ankylosis?
What is the main diagnostic feature of chronic osteomyelitis?
Which of the following is NOT true about HIV-associated osteomyelitis?
A patient with tubercular synovitis of the hip joint was treated with anti-tubercular therapy (ATT) and skin traction. Despite prolonged chemotherapy, no improvement is observed. What is the next best step in management?
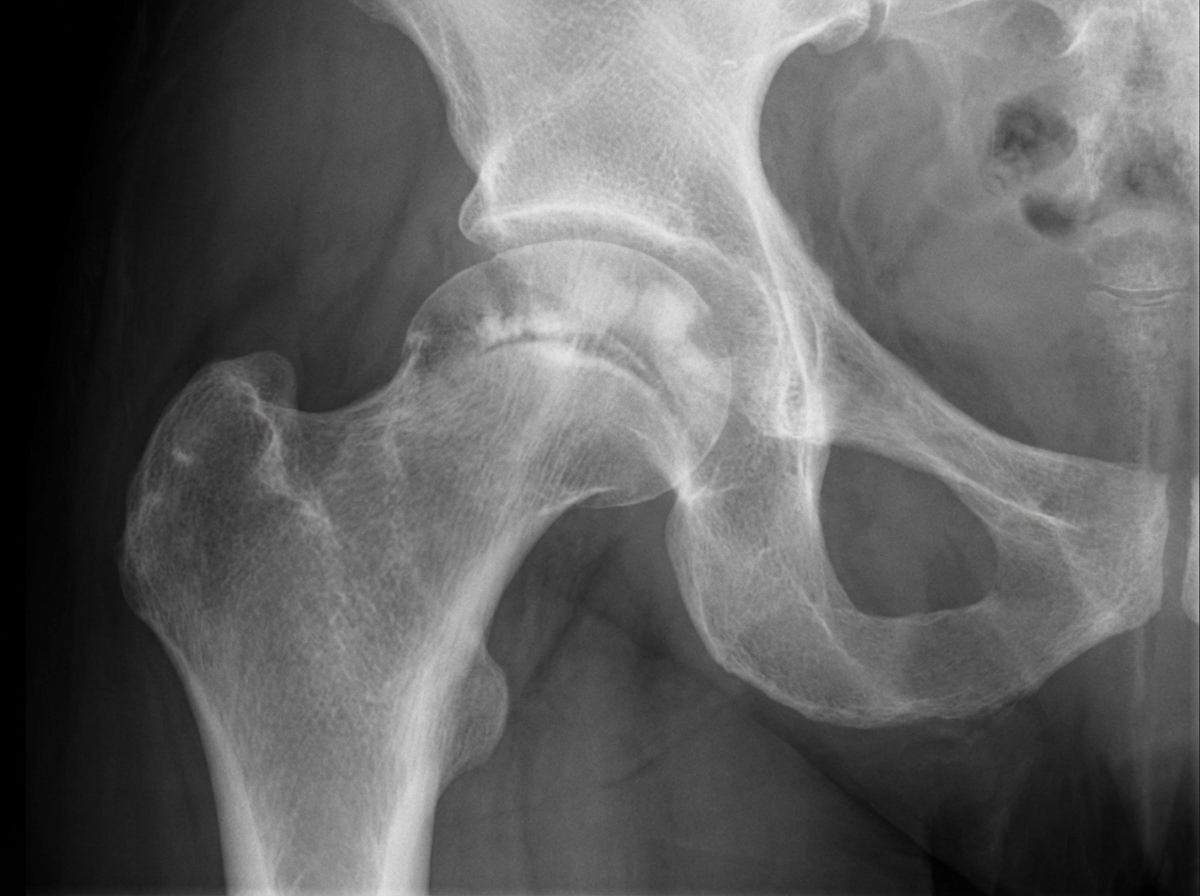
A 36-year-old woman with sickle cell disease presents with increasing pain in her right hip. She has no fever, chills, back or other bone pain, and there is no history of any trauma. On examination, her temperature is 37.3°C, range of motion in the right hip is reduced, she walks with a limp, and the right leg is shorter than the left. Movements of the hip and walking on it are painful. X-rays of the hip are shown. Which of the following is the most likely diagnosis?
Multifocal non-suppurative osteomyelitis is seen in which of the following conditions?
What is the most common site of tuberculosis?
Pseudoflexion deformity of the hip is typically seen in which of the following conditions?
Which of the following is NOT a deformity of rheumatoid arthritis?
What is true about synovial chondromatosis?
Practice by Chapter
Septic Arthritis
Practice Questions
Osteomyelitis
Practice Questions
Tuberculosis of Bones and Joints
Practice Questions
Fungal and Parasitic Infections
Practice Questions
Diabetic Foot Infections
Practice Questions
Prosthetic Joint Infections
Practice Questions
Reactive Arthritis
Practice Questions
Management of Joint Infections
Practice Questions
Prevention of Orthopaedic Infections
Practice Questions
Biofilms in Orthopaedic Infections
Practice Questions
Antibiotic Prophylaxis
Practice Questions
Implant-Related Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app