
Prenatal Care — MCQs

On this page
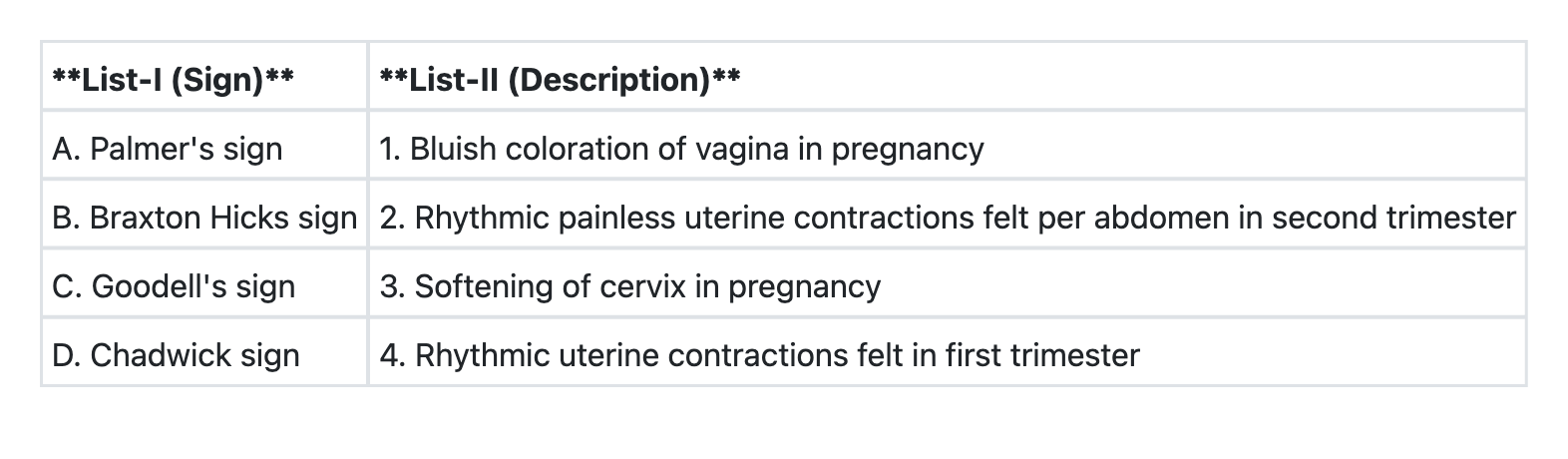
Match List-I with List-II and select the correct answer using the code given below the Lists:
Abnormally low alpha-fetoprotein in maternal serum indicates:
Which one of the following is NOT done as screening test in pregnancy?
The most common cause of early spontaneous abortion is:
The Maternal serum α-fetoprotein level is elevated in all EXCEPT:
In pregnancy with Down syndrome consider the following biomarkers: 1. β HCG is raised 2. α FP is raised 3. Inhibin A is decreased Which of the above statements is/are correct?
Which one of the following statements regarding pre-conceptional counseling is NOT correct?
A 23-year-old woman presents at 10 weeks gestation with a positive rapid plasma reagin (RPR) titer of 1:64 and positive TPHA. She was treated for primary syphilis 2 years ago with appropriate penicillin therapy, after which her RPR declined to 1:2. She denies any new symptoms or sexual contacts since then. What is the most appropriate management?
What is the most appropriate topical treatment for external genital warts in pregnancy?
A 34-year-old pregnant woman at 28 weeks gestation is found to have a positive treponemal test (TPHA) but negative non-treponemal test (VDRL) during routine antenatal screening. She has no history of syphilis treatment. What is the most appropriate interpretation and management?
Practice by Chapter
Preconception Counseling
Practice Questions
Pregnancy Diagnosis and Dating
Practice Questions
Routine Antenatal Assessments
Practice Questions
Maternal Physiological Changes
Practice Questions
Nutrition in Pregnancy
Practice Questions
Screening Tests in Pregnancy
Practice Questions
Fetal Growth Assessment
Practice Questions
High-Risk Pregnancy Identification
Practice Questions
Antenatal Complications Management
Practice Questions
Psychosocial Aspects of Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app