
Prenatal Care — MCQs

On this page
In the quadruple test conducted as a part of screening, which is the most likely indicator of maternal-fetal placental unit?
The maternal serum alpha-fetoprotein concentration is elevated in the following conditions except
While making a pelvic assessment in a gravid woman, the obstetrician can measure with examining finger the following diameter:
The daily requirement of calcium during normal pregnancy is
During a normal pregnancy, the changes occurring in the urinary tract include the following except
Serum AFP (alpha fetoprotein) levels are increased at 16 weeks of pregnancy in all the following conditions, except
A pregnant woman presents at 28 weeks of gestation with haemoglobin level of 7 gm%; and peripheral smear reveals it to be of microcytic hypochromic type. What would be the correct option of therapy?
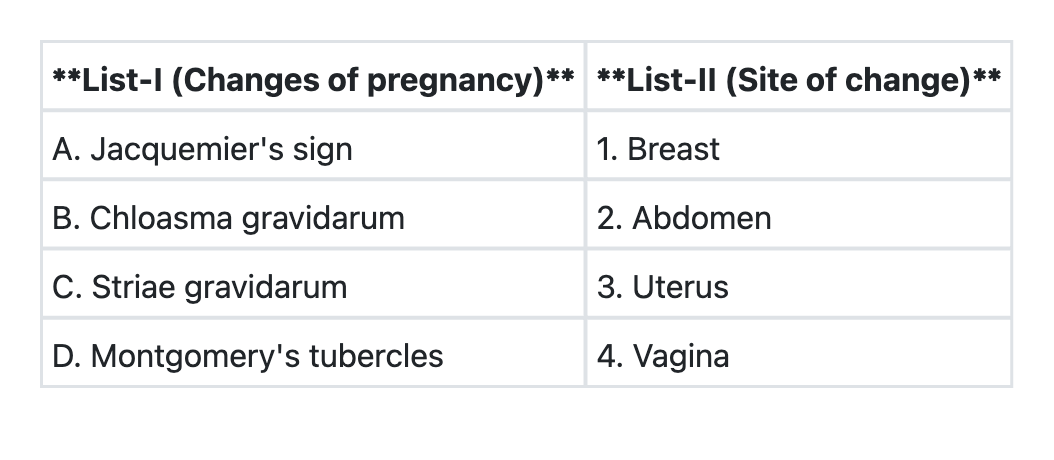
Match List-I (Signs of pregnancy) with List-II (Anatomical sites) and select the correct answer using the code given below the Lists:
In pregnancy, there is a physiological increase of the
Which of the following vaccines is/are contraindicated in pregnancy? 1. Rubella 2. Hepatitis-B 3. Diphtheria 4. Mumps 5. Measles Select the correct answer using the code given below:
Practice by Chapter
Preconception Counseling
Practice Questions
Pregnancy Diagnosis and Dating
Practice Questions
Routine Antenatal Assessments
Practice Questions
Maternal Physiological Changes
Practice Questions
Nutrition in Pregnancy
Practice Questions
Screening Tests in Pregnancy
Practice Questions
Fetal Growth Assessment
Practice Questions
High-Risk Pregnancy Identification
Practice Questions
Antenatal Complications Management
Practice Questions
Psychosocial Aspects of Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app