
Prenatal Care — MCQs

On this page
What is the most common complication of urinary tract infection (UTI) during pregnancy?
A woman comes to the clinic with breast tenderness, presence of linea nigra on her abdomen, and a bluish discoloration of the cervix. What is the most likely clinical interpretation of these findings?
A woman presents for her first antenatal visit and reports that her LMP was approximately 2 months ago. Which ultrasound parameter is the most accurate for dating the pregnancy at this stage?
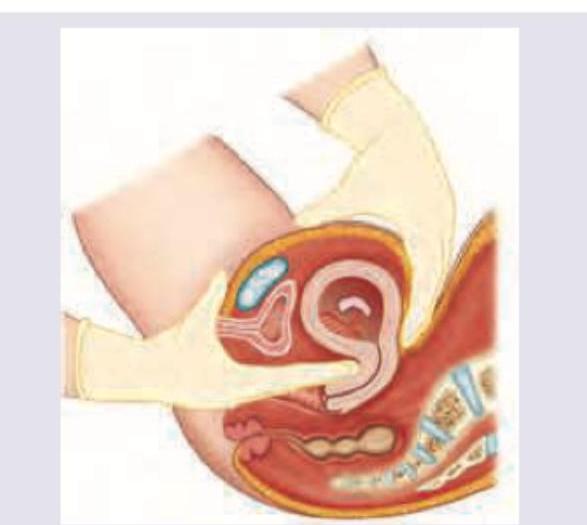
What is the clinical sign elicited?
The following USG scan should prompt you to screen for which of the following disorders?

Which of the following Leopold's grip is shown in the image?

The commonest ovarian tumour seen during pregnancy is:
Chadwick's sign describes :
Which of the following vaccines can be given to a pregnant woman ? 1. COVID vaccine 2. Measles, Mumps, Rubella vaccine 3. Hepatitis B vaccine 4. Rabies vaccine Select the correct answer using the code given below :
A typical case of Iron Deficiency Anaemia (IDA) in pregnancy will show which of the following? 1. Hb less than 10 g/dL 2. PCV less than 30% 3. MCHC more than 30% 4. Microcytic hypochromic picture on peripheral blood smear (PBS). Select the correct answer using the code given below:
Practice by Chapter
Preconception Counseling
Practice Questions
Pregnancy Diagnosis and Dating
Practice Questions
Routine Antenatal Assessments
Practice Questions
Maternal Physiological Changes
Practice Questions
Nutrition in Pregnancy
Practice Questions
Screening Tests in Pregnancy
Practice Questions
Fetal Growth Assessment
Practice Questions
High-Risk Pregnancy Identification
Practice Questions
Antenatal Complications Management
Practice Questions
Psychosocial Aspects of Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app