
Prenatal Care — MCQs

On this page
After an initial serum $\beta$-hCG test in a patient with suspected pregnancy, when should the repeat $\beta$-hCG level ideally be checked to assess viability or progression?
A 24-year-old primigravida presents with painful vaginal bleeding in the first trimester. On USG, a well-formed gestation ring with central echoes from the embryo indicates a healthy fetus, and there is observation of fetal cardiac motion. What is the most probable diagnosis?
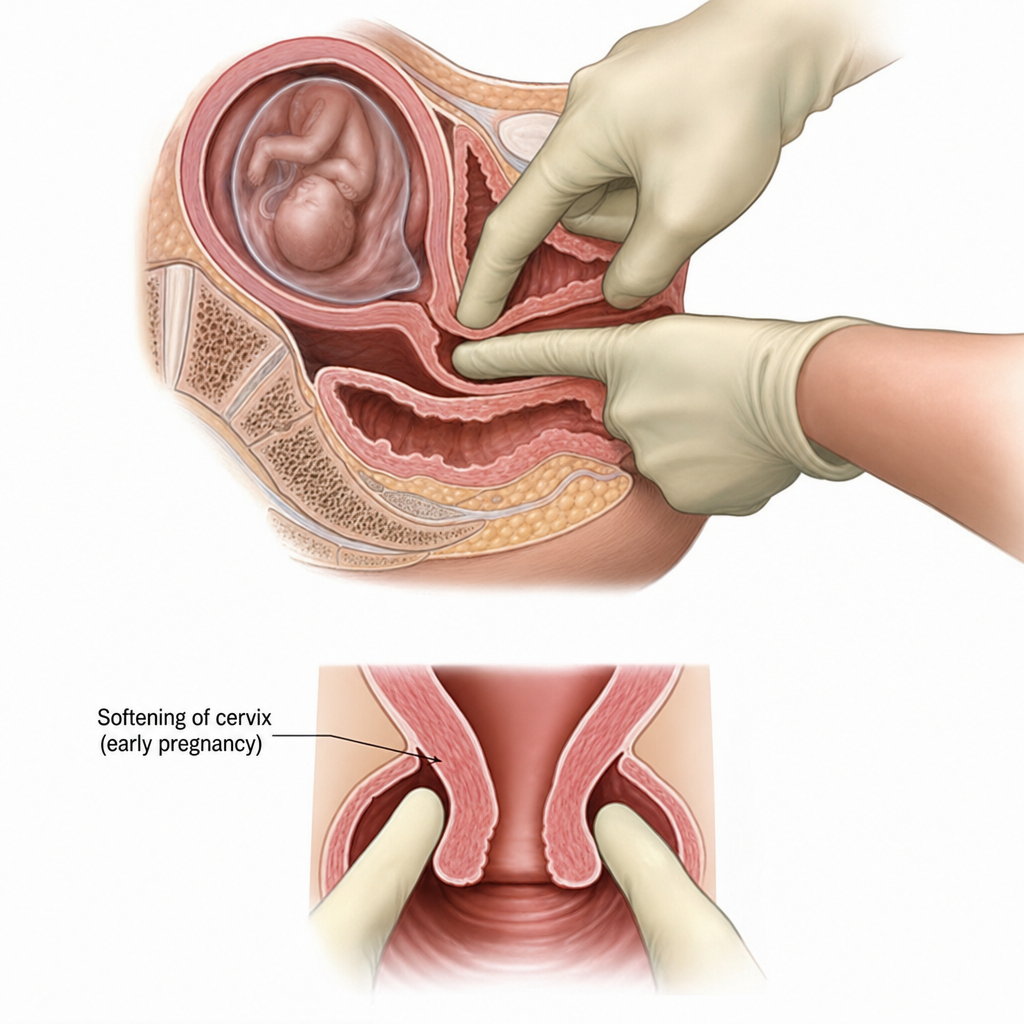
Identify the sign.
Which of the following CVS changes are not seen in pregnancy?
What is the earliest sign of pregnancy on TVS?
The image depicts which of the following early signs of pregnancy?
Which sign of pregnancy is demonstrated in the image below?
Which of the following is the best parameter for estimation of fetal age by ultrasound in 1st trimester?
Which of the following is shown in the given image? 
All of the following are true about audit in obstetrics except:
Practice by Chapter
Preconception Counseling
Practice Questions
Pregnancy Diagnosis and Dating
Practice Questions
Routine Antenatal Assessments
Practice Questions
Maternal Physiological Changes
Practice Questions
Nutrition in Pregnancy
Practice Questions
Screening Tests in Pregnancy
Practice Questions
Fetal Growth Assessment
Practice Questions
High-Risk Pregnancy Identification
Practice Questions
Antenatal Complications Management
Practice Questions
Psychosocial Aspects of Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app