
Prenatal Care — MCQs

On this page
What is the earliest structure detectable for pregnancy by ultrasound?
Which of the following is NOT used for antenatal screening?
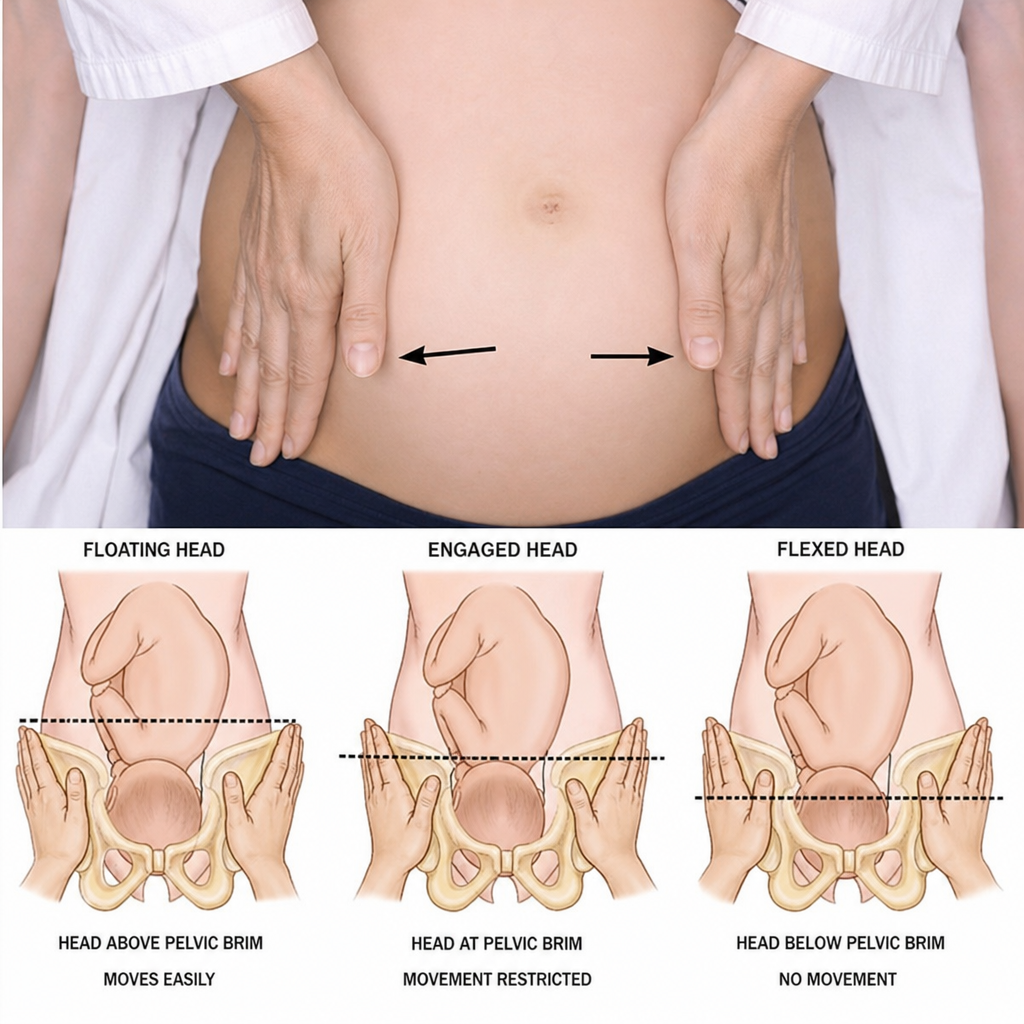
The maneuver shown below helps specifically in?
Which cardiovascular change is physiological in the last trimester of pregnancy?
The double decidual sac sign (DDSS) is the best ultrasound method for diagnosing which of the following?
What is true about hematological changes in pregnancy?
What is a common cardiovascular change observed during pregnancy?
What is the approximate fetal weight if the height of the uterus above the pubic symphysis is 35 cm and the station of the head is -2?
What is uterine souffle?
What is the minimum height for a primigravida woman to be considered for intervention regarding fetal growth?
Practice by Chapter
Preconception Counseling
Practice Questions
Pregnancy Diagnosis and Dating
Practice Questions
Routine Antenatal Assessments
Practice Questions
Maternal Physiological Changes
Practice Questions
Nutrition in Pregnancy
Practice Questions
Screening Tests in Pregnancy
Practice Questions
Fetal Growth Assessment
Practice Questions
High-Risk Pregnancy Identification
Practice Questions
Antenatal Complications Management
Practice Questions
Psychosocial Aspects of Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app