
Prenatal Care — MCQs

On this page
Which of the following is NOT true about femur length used as a fetal biometric measure?
Which clotting factor is not increased in pregnancy?
At what gestational age is the following procedure ideally performed?
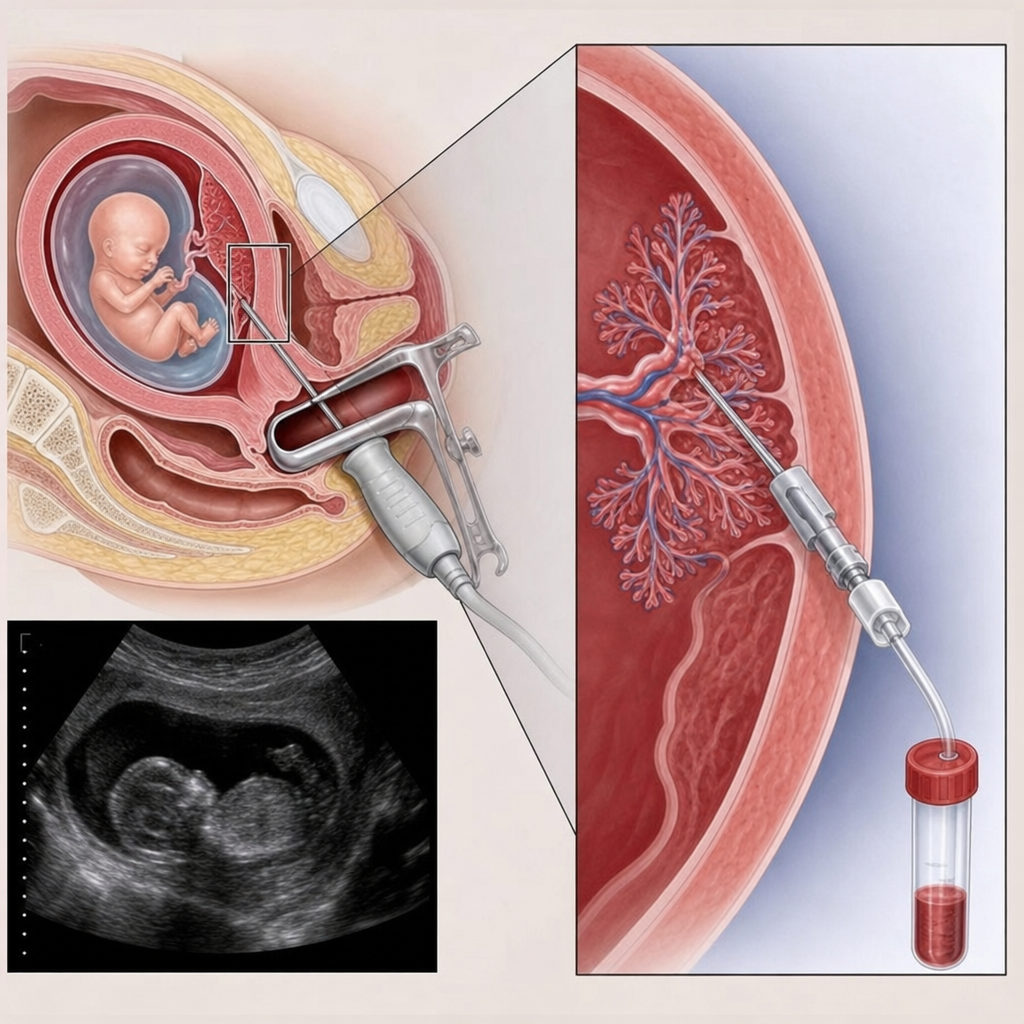
Which of the following statements is FALSE regarding chorionic villus sampling?
Which of the following changes that occur in the renal system during pregnancy is FALSE?
At what value for a one-hour glucose challenge test would you recommend a standard glucose tolerance test?
Which of the following embryonic structures is the earliest ultrasonographically visible indicator of pregnancy?
A 23-year-old female presents with a missed menstrual period of two cycles and a positive urine pregnancy test. Ultrasound confirms a 12-week gestation. She is concerned because she received the Measles Mumps Rubella (MMR) vaccine four months prior to conception, having been advised to wait three months before conceiving. The pregnancy is desired. What is the most appropriate next step?
If a fetus has Down syndrome, what finding will NOT be shown on a quadruple marker screening test?
Which test has the fastest lab processing time for karyotype assessment?
Practice by Chapter
Preconception Counseling
Practice Questions
Pregnancy Diagnosis and Dating
Practice Questions
Routine Antenatal Assessments
Practice Questions
Maternal Physiological Changes
Practice Questions
Nutrition in Pregnancy
Practice Questions
Screening Tests in Pregnancy
Practice Questions
Fetal Growth Assessment
Practice Questions
High-Risk Pregnancy Identification
Practice Questions
Antenatal Complications Management
Practice Questions
Psychosocial Aspects of Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app