
Prenatal Care — MCQs

On this page
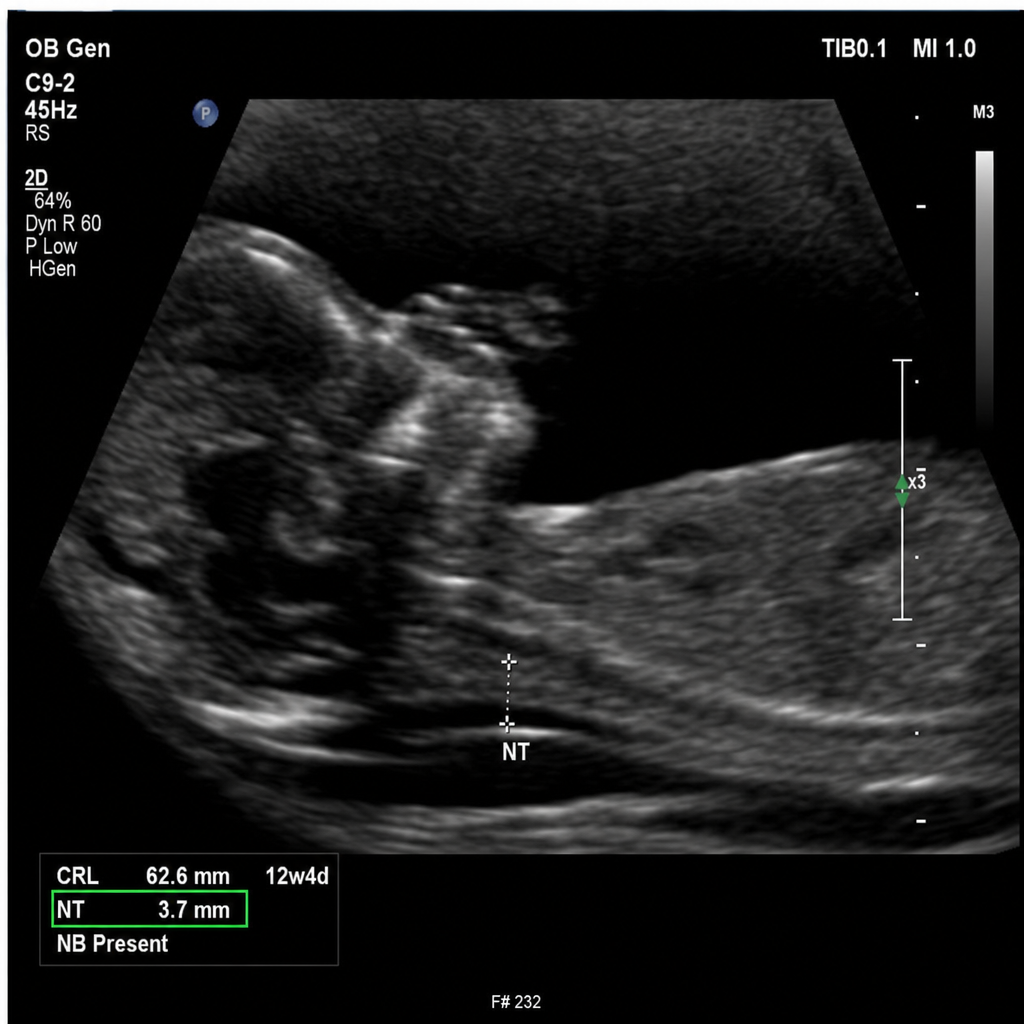
Which of the following is an exception to the guidelines for correct Nuchal translucency measurement?
A 23-year-old woman at 10 weeks' gestation presents for her initial evaluation. She has a history of asthma exacerbations requiring hospitalization but has never needed intubation or intensive care unit admission. Her asthma is controlled with daily inhaled corticosteroids and albuterol, providing adequate symptom relief. She is concerned about continuing these medications during pregnancy. Which of the following is true regarding asthma medications in pregnancy?
Which of the following vaccines is NOT contraindicated in pregnancy?
What is the most accurate method of diagnosing pregnancy at 6 weeks?
What is the primary treatment for red degeneration of a fibroid during pregnancy?
An ultrasound measures a parameter at 3.7 mm. What does this measurement indicate?
What is the appropriate management of vulvar varices during pregnancy?
A gravida 2 with 1 normal live birth has presented to the clinic with a transverse lie at 36 weeks gestation. What should be the next step of management in this patient?
What does Goodell's sign indicate?
To obtain true conjugate, what factor should be subtracted from the diagonal conjugate?
Practice by Chapter
Preconception Counseling
Practice Questions
Pregnancy Diagnosis and Dating
Practice Questions
Routine Antenatal Assessments
Practice Questions
Maternal Physiological Changes
Practice Questions
Nutrition in Pregnancy
Practice Questions
Screening Tests in Pregnancy
Practice Questions
Fetal Growth Assessment
Practice Questions
High-Risk Pregnancy Identification
Practice Questions
Antenatal Complications Management
Practice Questions
Psychosocial Aspects of Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app