
Virology — MCQs

On this page
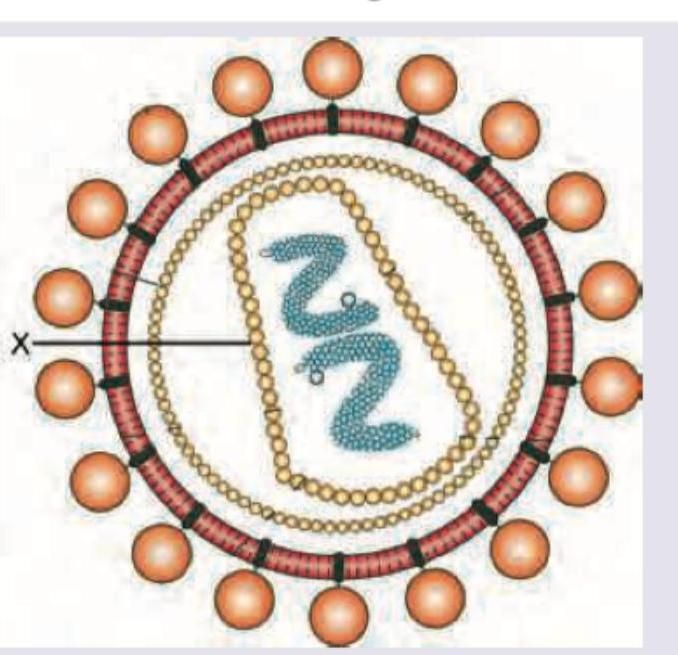
Name the antigen marked X in the figure:
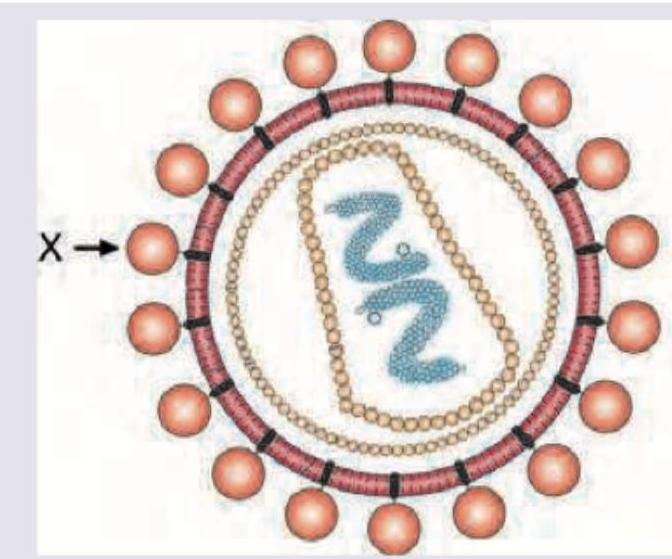
Comment on the marking X in HIV virus.
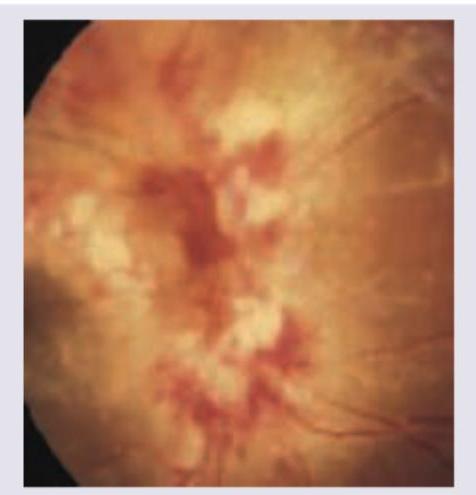
A 40-year-old AIDS positive patient complains of seeing floaters followed by progressive reduction in visual acuity over next weeks. Fundus examination was performed. All are true about the causative agent except: (Recent NEET Pattern 2016-17)
A 2-year-old unimmunized child from a village presents with fever, decreased feeding and ear ache. All are true about the virus responsible for the condition shown except: (Recent NEET Pattern 2016-17)

A 3-year-old child presents with fever for 3 days with excessive salivation. On examination following lesions were seen. Mother says same lesions appeared 6 months back. All are true about the condition shown except:

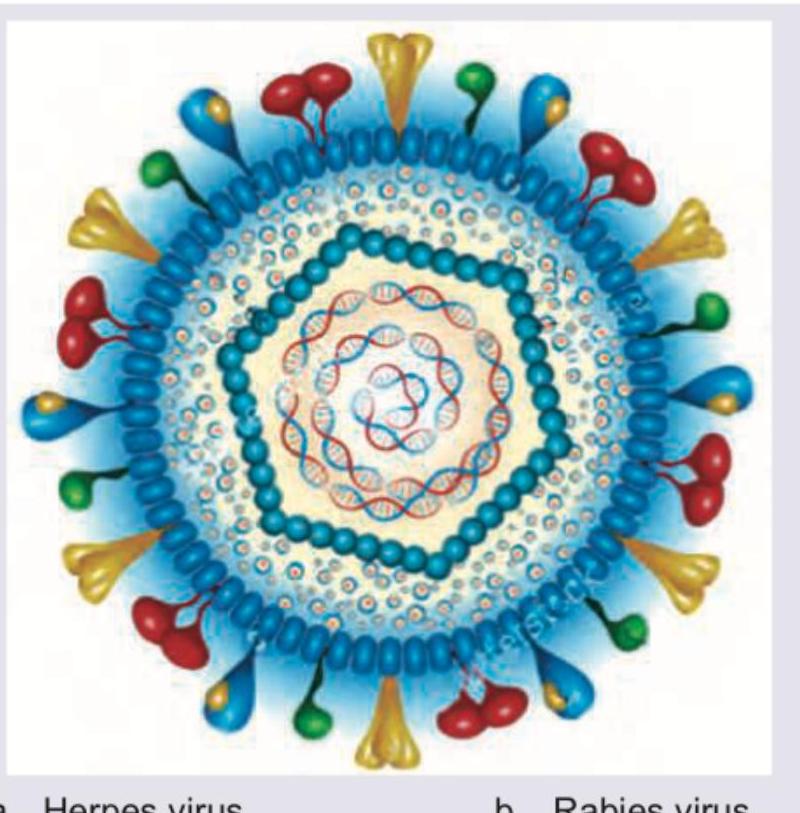
The schematic is intended to represent a herpesvirus; the coiled appearance of the nucleic acid is illustrative and does not indicate genome topology. Which description correctly characterizes a herpesvirus virion?
Which of the following diseases is caused by the virus shown below?

Which of the following diseases is caused by the virus shown below?
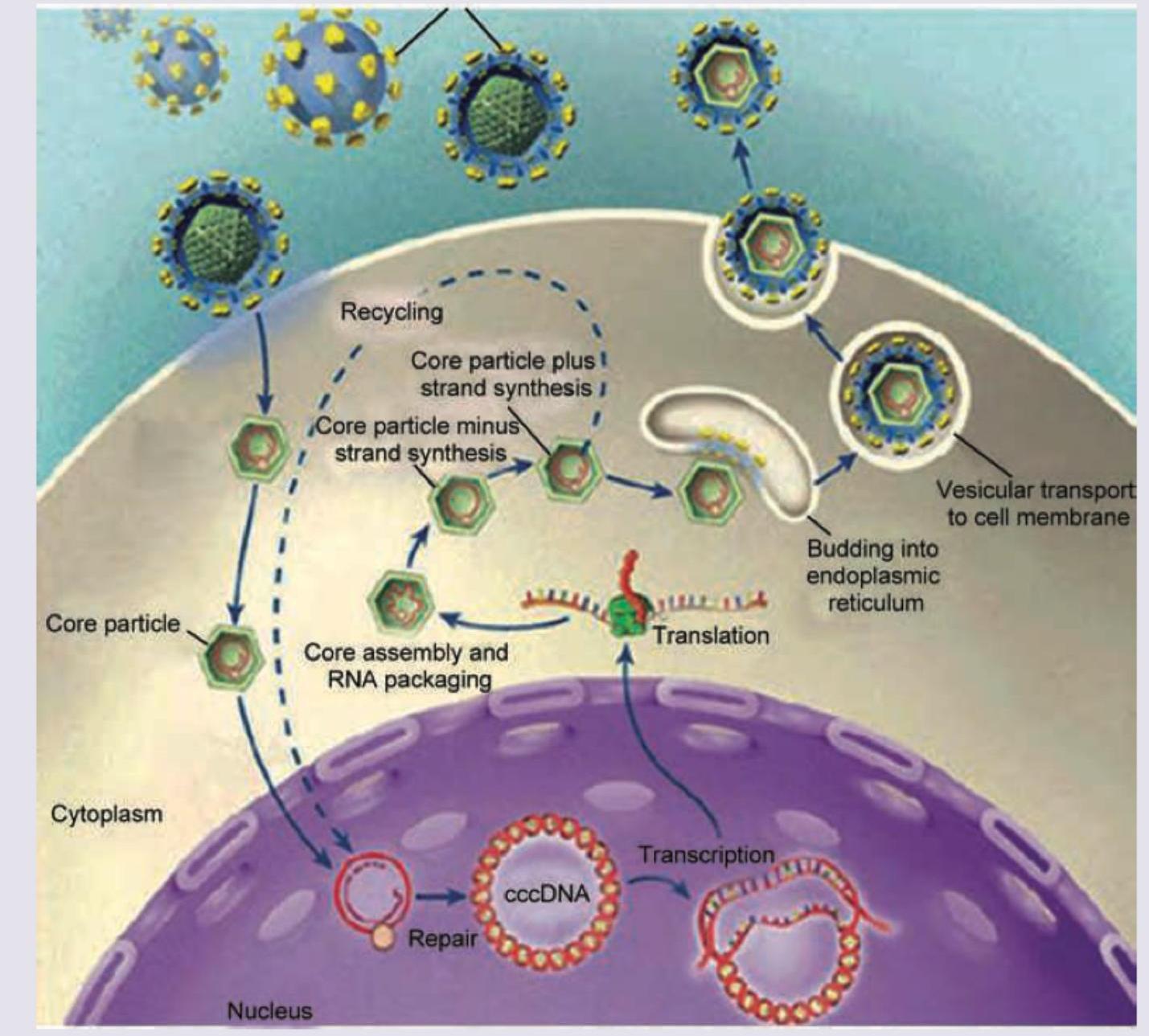
Amongst the four choices, select the virus whose life cycle is shown. (AIIMS Nov 2017)
Which of the following is responsible for the abnormality shown below?

Practice by Chapter
Virus Structure and Classification
Practice Questions
Viral Replication
Practice Questions
Pathogenesis of Viral Infections
Practice Questions
DNA Viruses: Herpesviruses
Practice Questions
DNA Viruses: Poxviruses and Adenoviruses
Practice Questions
Hepatitis Viruses
Practice Questions
RNA Viruses: Orthomyxoviruses
Practice Questions
RNA Viruses: Paramyxoviruses
Practice Questions
Enteroviruses and Rhinoviruses
Practice Questions
Arboviruses
Practice Questions
HIV and Retroviruses
Practice Questions
Oncogenic Viruses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app