
Virology — MCQs

On this page
Receptor used for the entry of HIV virus into the host cell is?
A child was brought with c/o multiple lesions. O/E multiple vesicular lesions are seen on the palms, soles, and oral mucosa. Which of the following is the most likely etiological agent causing the disease?
A patient is positive for HBsAg and anti-HBc IgM. What is the most likely diagnosis?
Which of the following hepatitis viruses is likely to get transmitted via fecal-oral route?
The image shown here is used for the diagnosis of a virus belonging to which family?
Acute hemorrhagic conjunctivitis is caused by which of the following combinations?
A young adult presents with facial pain and painful vesicular lesions in the mouth. Tzanck smear reveals multinucleated giant cells with intranuclear inclusions. What is the most likely causative organism?
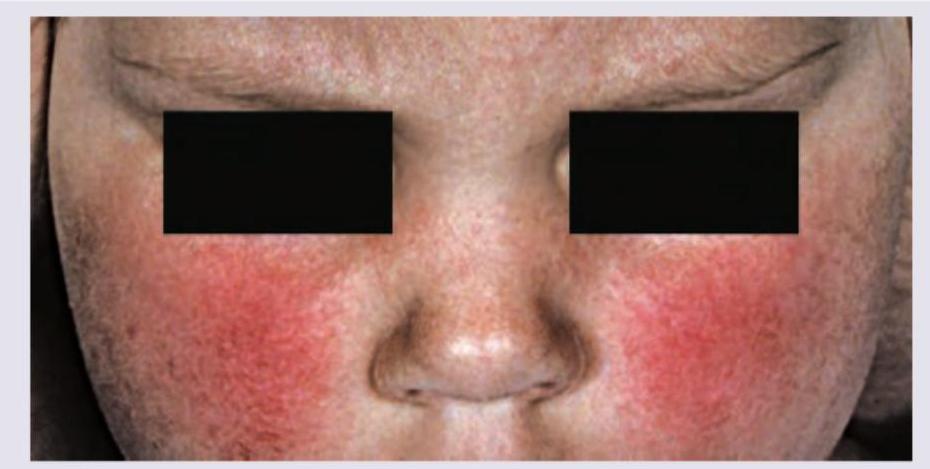
The following disease presentation is caused by:
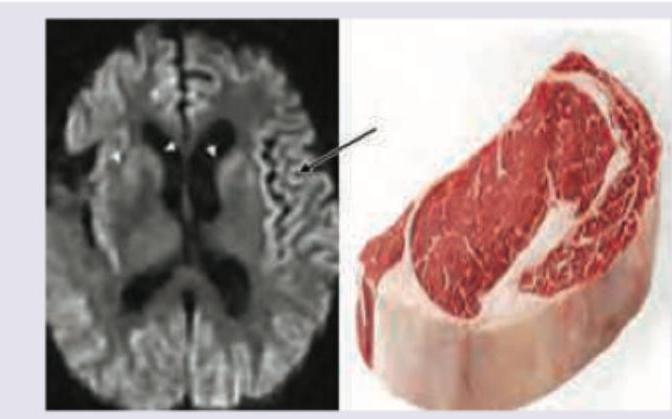
A 25-year-old abattoir worker presents with myoclonus and amnesia for recent and remote events for last 1 year. MRI head was performed. All statements are correct about the infectious agent leading to this disease except:
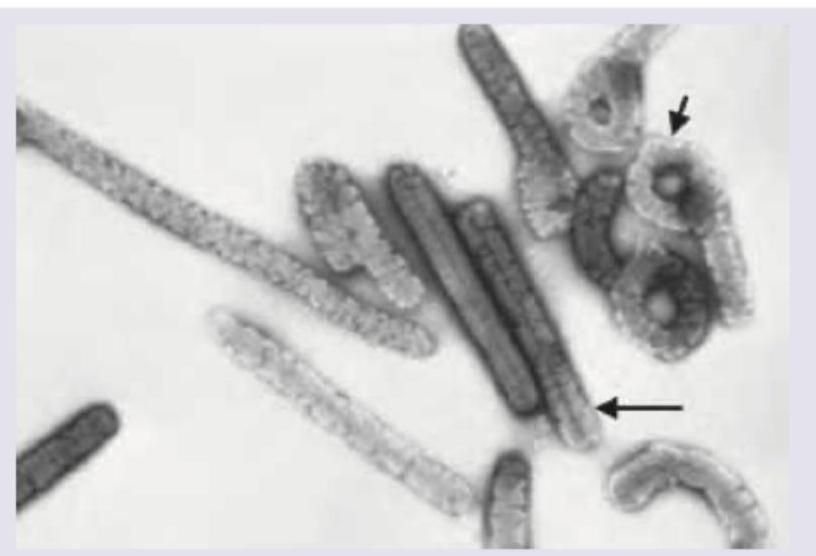
The following electron microscope image shows presence of:
Practice by Chapter
Virus Structure and Classification
Practice Questions
Viral Replication
Practice Questions
Pathogenesis of Viral Infections
Practice Questions
DNA Viruses: Herpesviruses
Practice Questions
DNA Viruses: Poxviruses and Adenoviruses
Practice Questions
Hepatitis Viruses
Practice Questions
RNA Viruses: Orthomyxoviruses
Practice Questions
RNA Viruses: Paramyxoviruses
Practice Questions
Enteroviruses and Rhinoviruses
Practice Questions
Arboviruses
Practice Questions
HIV and Retroviruses
Practice Questions
Oncogenic Viruses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app