
Virology — MCQs

On this page
Regarding prions, which of the following statements is true?
Which of the following best explains why hepatitis C is the most common cause of posttransfusion hepatitis?
Which co-receptor is utilized by the R5 variant of the Human Immunodeficiency Virus?
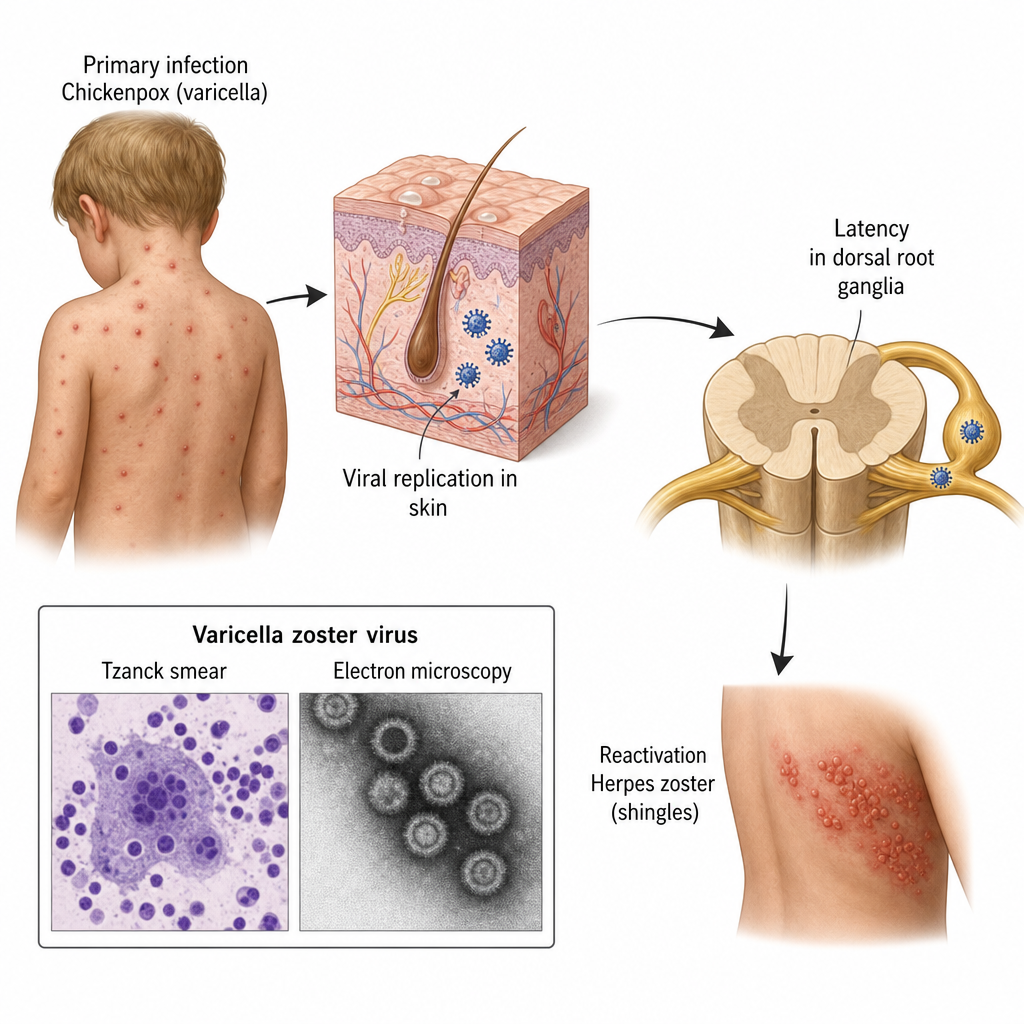
Varicella-zoster virus (VZV) is the cause of chickenpox and herpes zoster. Which of the following statements regarding VZV are true? a) Primary infection causes Varicella (Chickenpox) b) It remains latent in the B-cells c) Reactivation causes Herpes Zoster (Shingles) d) Post-herpetic neuralgia is a complication e) Live attenuated vaccine is available
Epstein-Barr virus (EBV) enters B-cells through which receptor?
Which of the following viruses does not have an envelope containing hemagglutinin or neuraminidase?
Herpangina is caused by which virus?
A dentist presents with pain, redness, and swelling of the finger, accompanied by fever. Examination reveals small, grouped vesicles containing clear fluid. A Tzanck smear shows Tzanck cells. What is the causative agent?
"Henderson-Patterson" bodies are seen in which of the following conditions?
Presence of HBeAg in serum of a patient of hepatitis-B indicates which stage?
Practice by Chapter
Virus Structure and Classification
Practice Questions
Viral Replication
Practice Questions
Pathogenesis of Viral Infections
Practice Questions
DNA Viruses: Herpesviruses
Practice Questions
DNA Viruses: Poxviruses and Adenoviruses
Practice Questions
Hepatitis Viruses
Practice Questions
RNA Viruses: Orthomyxoviruses
Practice Questions
RNA Viruses: Paramyxoviruses
Practice Questions
Enteroviruses and Rhinoviruses
Practice Questions
Arboviruses
Practice Questions
HIV and Retroviruses
Practice Questions
Oncogenic Viruses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app