
Virology — MCQs

On this page
An 18-year-old lady presents with severe sore throat, fever, and malaise. She has cervical lymphadenopathy, splenomegaly, and scattered petechiae on the soft palate with enlarged tonsils covered with white exudates. Which of the following investigations is most likely to help guide your management?
Pleomorphism is seen in which of the following conditions?
Varicella zoster virus remains latent in which of the following locations?
Which of the following is NOT a general property of viruses?
Which of the following diagnostic tests is NOT useful for its corresponding purpose?
Viruses grow well on which of the following?
Herpes simplex virus is classified as which of the following?
Condyloma acuminatum is caused by which types of Human Papillomavirus (HPV)?
A 2-year-old child attending daycare develops diarrhea and gastroenteritis as a result of adenoviral infection. Which of the following adenoviral serotypes would most likely be responsible for this child's illness?
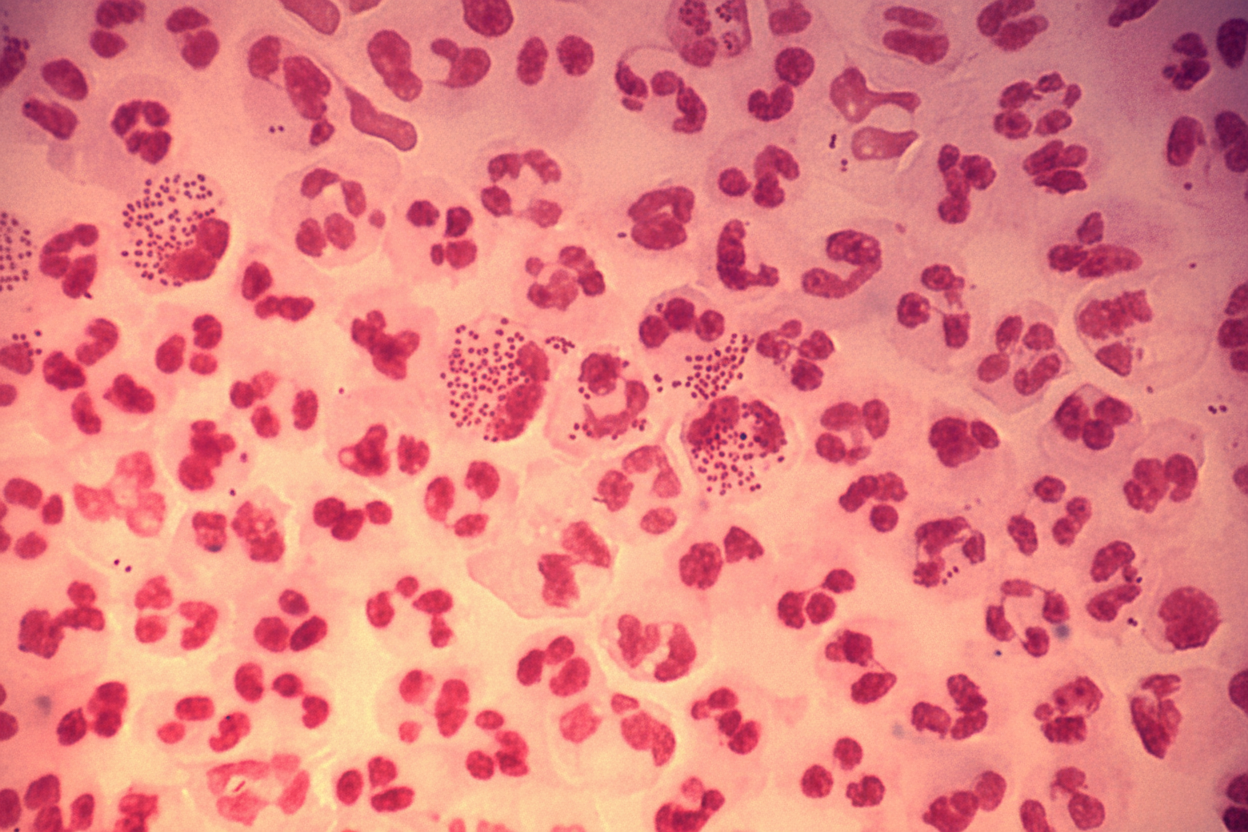
A 35-year-old male presents with a history of urethral discharge for the last three days. A Gram stain smear of the discharge is shown. Which of the following is true regarding the likely etiology?
Practice by Chapter
Virus Structure and Classification
Practice Questions
Viral Replication
Practice Questions
Pathogenesis of Viral Infections
Practice Questions
DNA Viruses: Herpesviruses
Practice Questions
DNA Viruses: Poxviruses and Adenoviruses
Practice Questions
Hepatitis Viruses
Practice Questions
RNA Viruses: Orthomyxoviruses
Practice Questions
RNA Viruses: Paramyxoviruses
Practice Questions
Enteroviruses and Rhinoviruses
Practice Questions
Arboviruses
Practice Questions
HIV and Retroviruses
Practice Questions
Oncogenic Viruses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app