
Virology — MCQs

On this page
Which dengue serotype has a higher risk of causing Dengue hemorrhagic fever as a secondary infection?
A 32-year-old unvaccinated woman presented with fever, headache, malaise, and ear pain along with parotid gland swelling. A week later, her fever resolved, but she developed pelvic pain and tenderness. Which virus is the likely causative agent?
RSV causes all EXCEPT:
1% silver nitrate is used for:
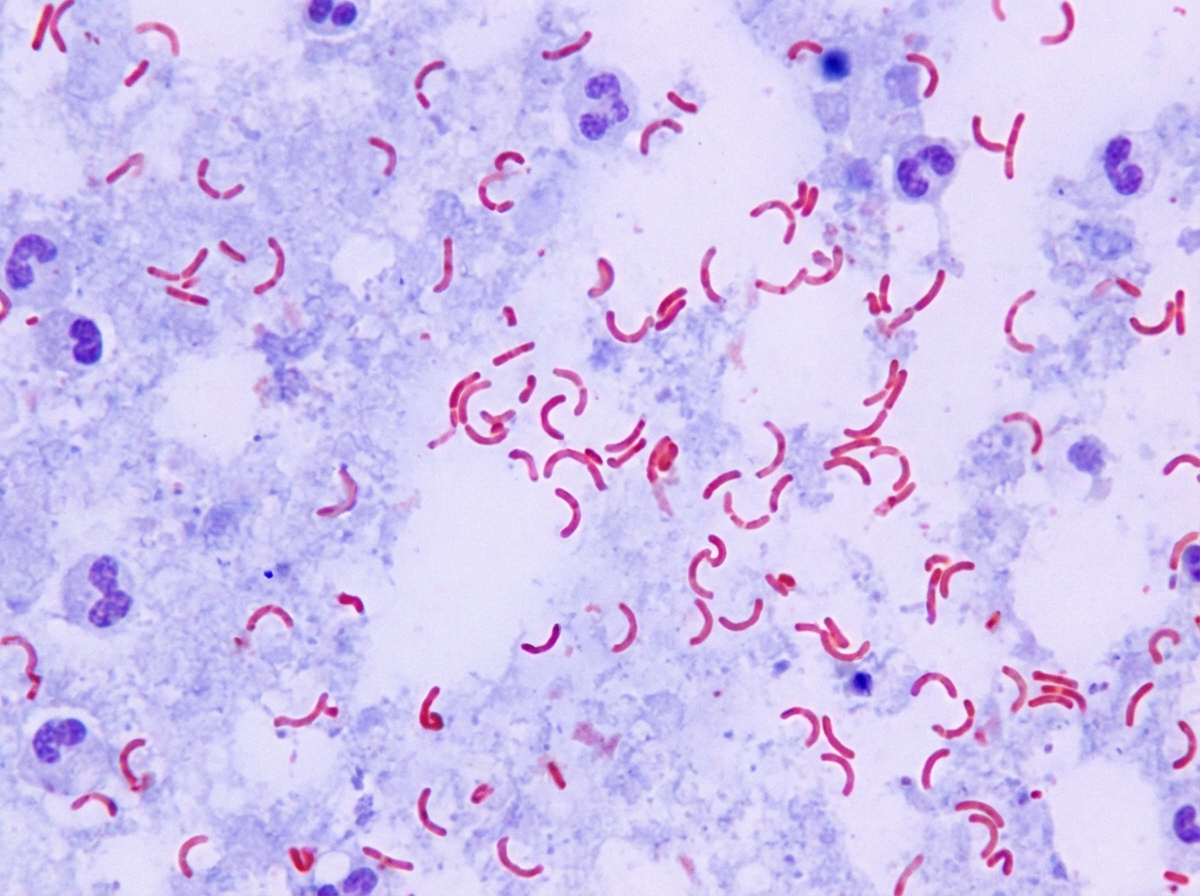
The following gram stain shows which bacteria?
Conjunctivitis is caused by all EXCEPT:
All are false regarding poliovirus except:
In HIV infection, gp120 envelope glycoproteins bind specifically to which cells?
All of the following statements are true regarding poliovirus except?
Which of the following conditions is NOT associated with Human Herpesvirus 8 (HHV-8)?
Practice by Chapter
Virus Structure and Classification
Practice Questions
Viral Replication
Practice Questions
Pathogenesis of Viral Infections
Practice Questions
DNA Viruses: Herpesviruses
Practice Questions
DNA Viruses: Poxviruses and Adenoviruses
Practice Questions
Hepatitis Viruses
Practice Questions
RNA Viruses: Orthomyxoviruses
Practice Questions
RNA Viruses: Paramyxoviruses
Practice Questions
Enteroviruses and Rhinoviruses
Practice Questions
Arboviruses
Practice Questions
HIV and Retroviruses
Practice Questions
Oncogenic Viruses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app