
Malaria Parasites — MCQs

Which of the following is detected in a peripheral blood smear?
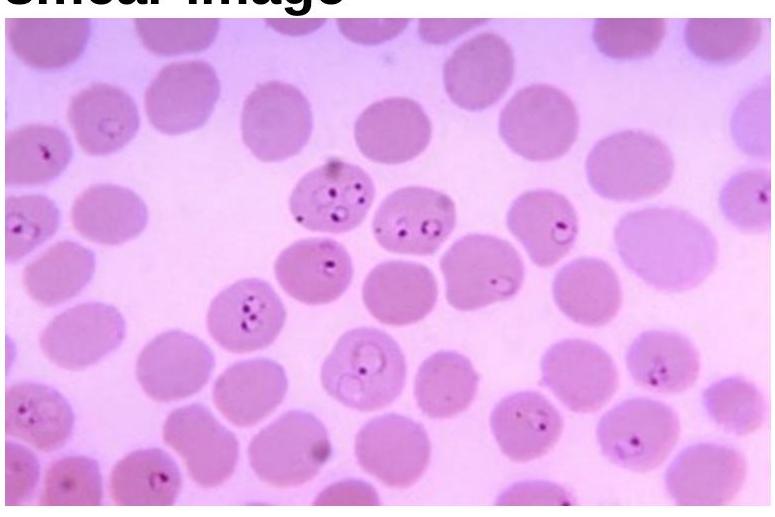
A boy presented with a fever and chills. Rapid test was positive for specific antigen HRP-2. Which of the following species of Plasmodium is the most likely causative agent?
Which of the following is the most appropriate treatment for a child with severe falciparum malaria with high parasitemia?
Which of the following is a chronic complication of malaria?
A person wants to visit a malaria endemic area of low level chloroquine resistant falciparum malaria. The best chemoprophylaxis is -
Which of the following statements about malaria transmission is correct?
Chemoprophylaxis of malaria can be done by all except:
Peripheral blood smear in Plasmodium falciparum infection may show all of the following except -
All of the following are seen in cerebral malaria, except:
Identify the organism related to the blood smear image.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app