
Intestinal Protozoa — MCQs

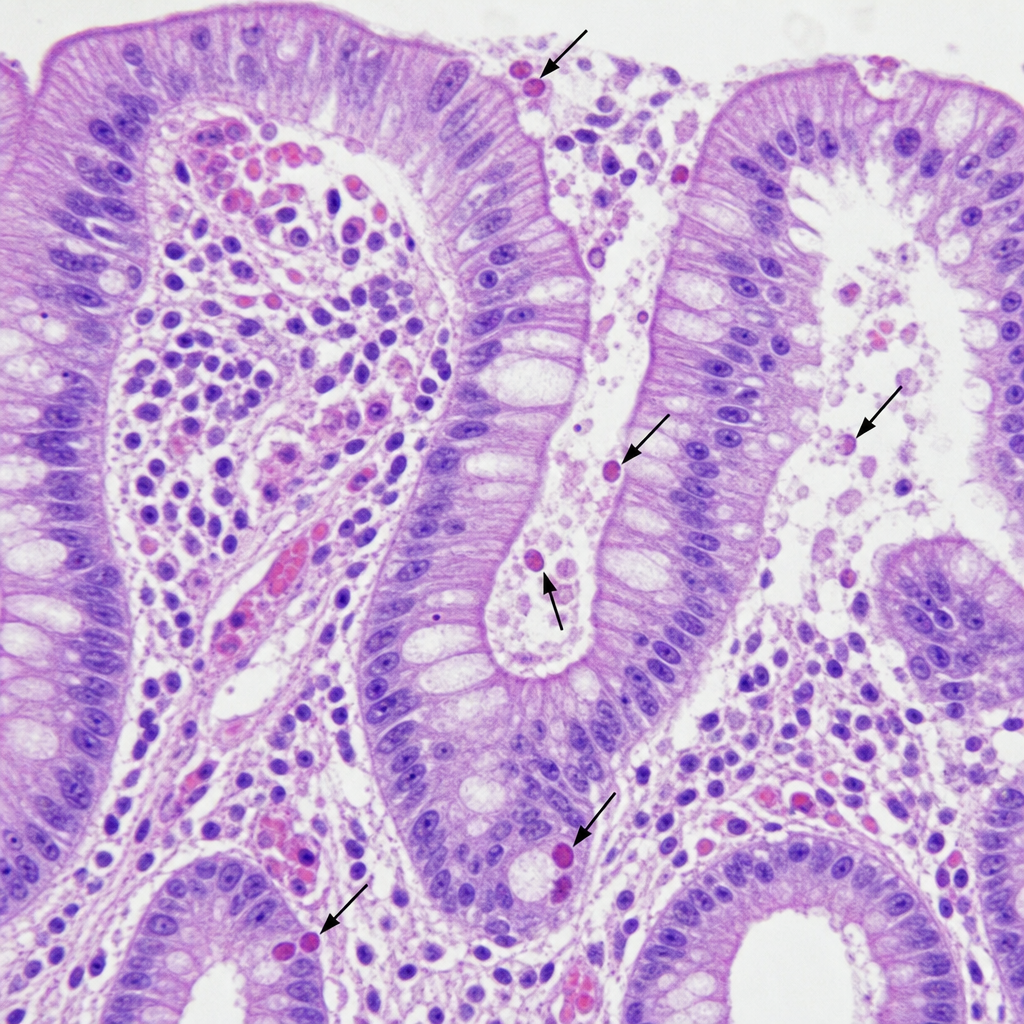
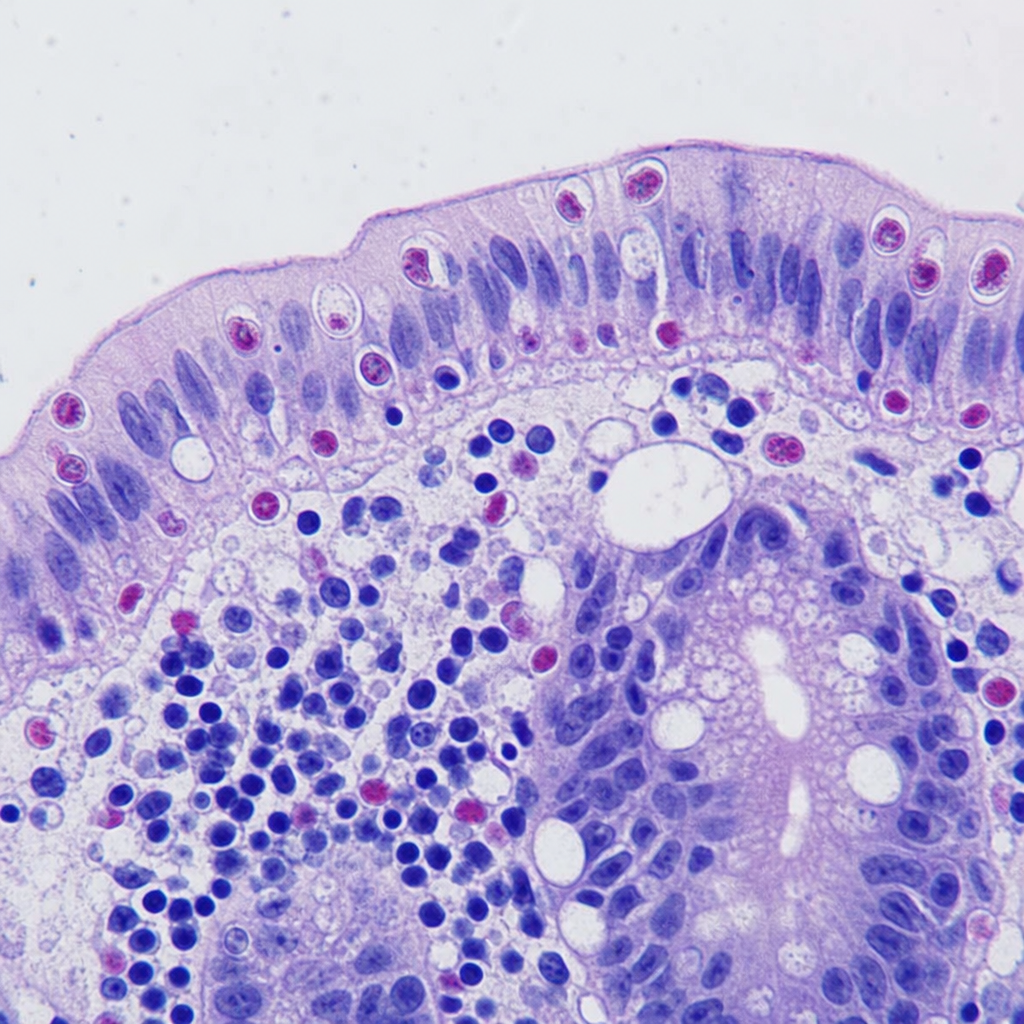
A 35-year-old heterosexual patient diagnosed with HIV presents with watery diarrhea. The colonoscopic biopsy is shown below. Which of the following is your most probable diagnosis?
A 30-year-old man with HIV presents with chronic diarrhea. Stool examination reveals small, spherical, acid-fast oocysts. What is the causative agent?
Amoebic liver abscess can be diagnosed by demonstrating-
Which of the following is the MOST characteristic clinical feature of Giardiasis?
A 4 year old child presents with acute watery diarrhea and abdominal cramps. Stool microscopy reveals trophozoites with falling leaf motility. What is the etiological agent?
A 6-year-old child is brought with high fever with rigors for 5 days with pain in right hypochondrium. On examination, the patient is anicteric and tenderness is noted in right upper quadrant. What is the best investigation for this case?
A known HIV patient on anti-retroviral therapy presented with diarrhea of six months duration. Stool microscopy showed 10-30 micrometer cysts, Kinyoun stain was positive. What is the most likely diagnosis?
A 35-year-old HIV positive patient comes with intractable diarrhea, crampy abdominal pain and vomiting. Biopsy of small intestine was taken which shows oocysts <10 µm as given below. What is the appropriate diagnosis?
A 15-year-old boy returned from a vacation to his relatives' village. He developed a severe headache and purulent nasal discharge and was diagnosed with primary amebic meningoencephalitis (PAM). He died 5 days later. Which is the most likely etiological agent?
Flask-shaped ulcers in the intestine are caused by which of the following?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app