
Mycology — MCQs

On this page
Which of the following statements regarding Candida are true?
A 34-week pregnant female presented with intense itching over the vulvar area and a white, cheesy vaginal discharge. On examination, vulvar erythema is noted. Which among the following is the causative organism in this patient?
Which of the following is not an opportunistic infection in AIDS?
A 24-year-old man is diagnosed with disseminated histoplasmosis after developing symptoms of fever, lymphadenopathy, hepatosplenomegaly, and pancytopenia. Which of the following is the body's major immunologic defense against histoplasmosis?
What is the primary site of infection in Cryptococcosis?
The organism most frequently related to mediastinal fibrosis is?
A section of tissue from the foot of a person with Eumycotic mycetoma shows a white, lobulated granule composed of fungal hyphae. What is the most common etiologic agent of this condition?
Discharging sinus is seen in which of the following conditions?
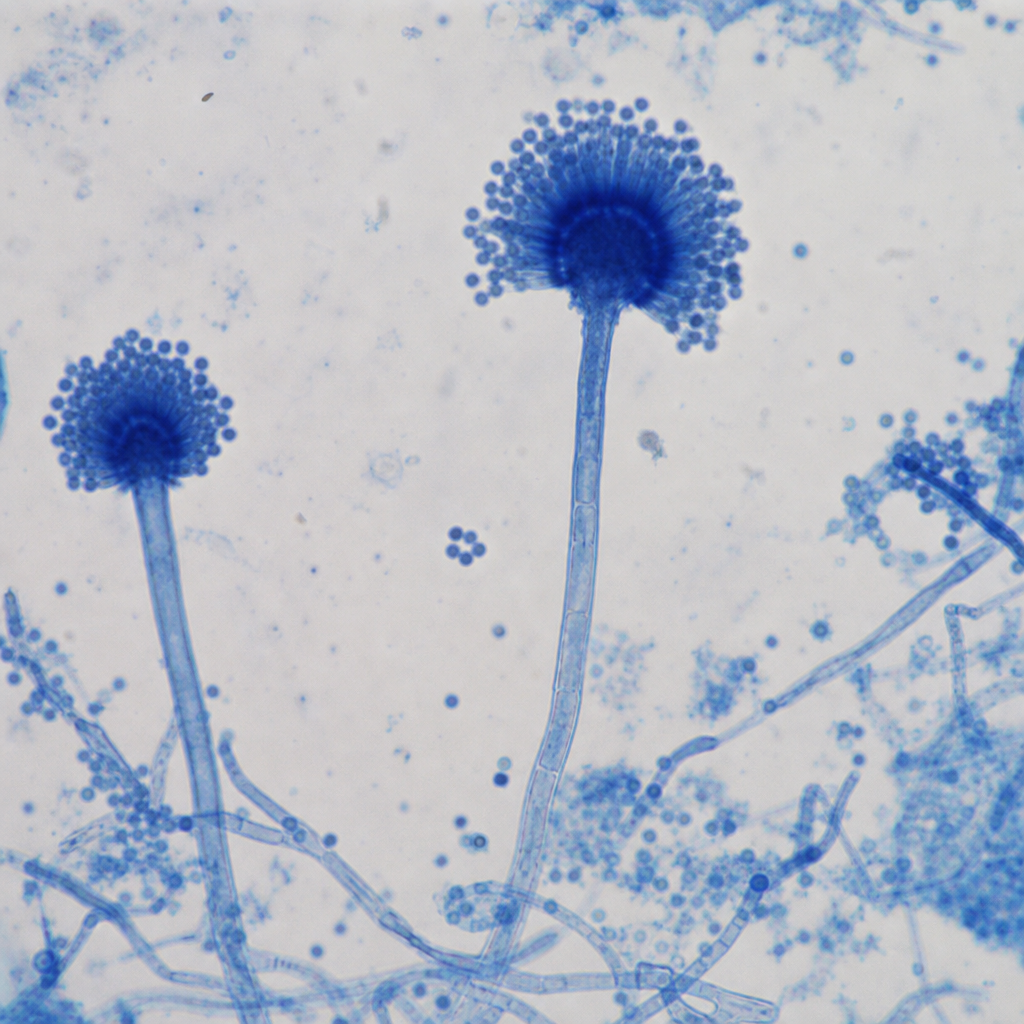
The organism shown below is:
Which of the following statements about dermatophytes is FALSE?
Practice by Chapter
Classification of Fungi
Practice Questions
Superficial Mycoses
Practice Questions
Dermatophytes
Practice Questions
Subcutaneous Mycoses
Practice Questions
Candidiasis
Practice Questions
Aspergillosis
Practice Questions
Cryptococcosis
Practice Questions
Zygomycosis
Practice Questions
Endemic Mycoses
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Antifungal Agents
Practice Questions
Laboratory Diagnosis of Fungal Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app