
Mycology — MCQs

On this page
A person came with the H/o thorn prick a week ago. A few days later, he developed ulcers along lymphatic drainage. Choose the correct organism.
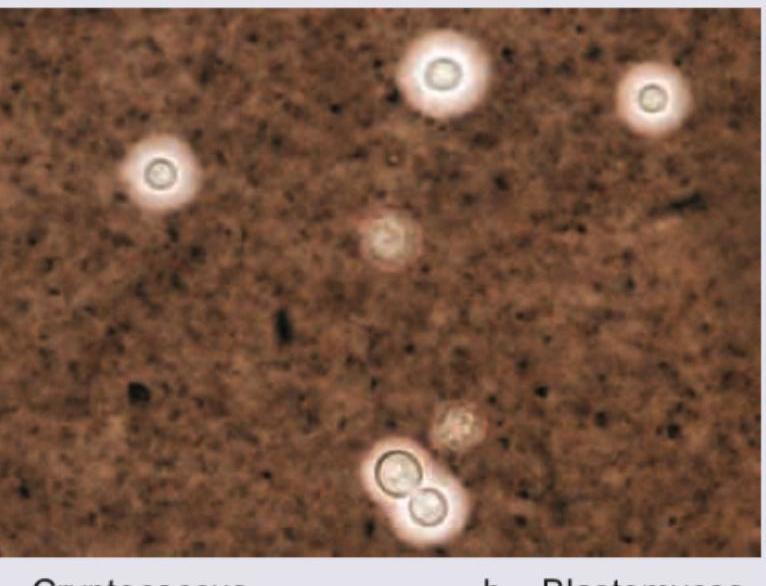
A 39-year-old patient with HIV and a CD4 count of 139 cells/μL presents with altered sensorium and impaired consciousness. CSF examination using an India ink preparation reveals a positive result. Which organism is most likely responsible?
Which of the following dimorphic fungi causes subcutaneous mycosis?
The stain used for identifying Cryptococcus is
A 35-year-old female presents with vaginal discharge and vulvar itching. Wet mount examination shows budding yeast cells with pseudohyphae. Vaginal pH is 4.5. What is the most likely causative organism?
All of the following are dimorphic fungi except:
A white patch is observed in the oral cavity of an immunocompromised patient. Which of the following findings is most likely on microscopy?
A patient presents with low-grade fever, chronic cough, and weight loss. Fungal culture from respiratory secretions shows the following organism with characteristic tuberculate macroconidia on microscopy. What is the most likely diagnosis?
A patient presents with irregular swelling over the foot, multiple discharging sinuses, and black granules. A KOH mount is performed on the discharge. What is the most likely observation?
A patient presented with headache and projectile vomiting and altered sensorium. The following organism was demonstrated on India ink staining. What is the likely diagnosis?
Practice by Chapter
Classification of Fungi
Practice Questions
Superficial Mycoses
Practice Questions
Dermatophytes
Practice Questions
Subcutaneous Mycoses
Practice Questions
Candidiasis
Practice Questions
Aspergillosis
Practice Questions
Cryptococcosis
Practice Questions
Zygomycosis
Practice Questions
Endemic Mycoses
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Antifungal Agents
Practice Questions
Laboratory Diagnosis of Fungal Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app