
Mycology — MCQs

On this page
Oral candidiasis can be classified as primary and _____ based on underlying predisposing factors:
The yeast which shows thick gelatinous capsule and positive for mucicarmine is
Which organism does not affect hair?
Dermatophytes affect -
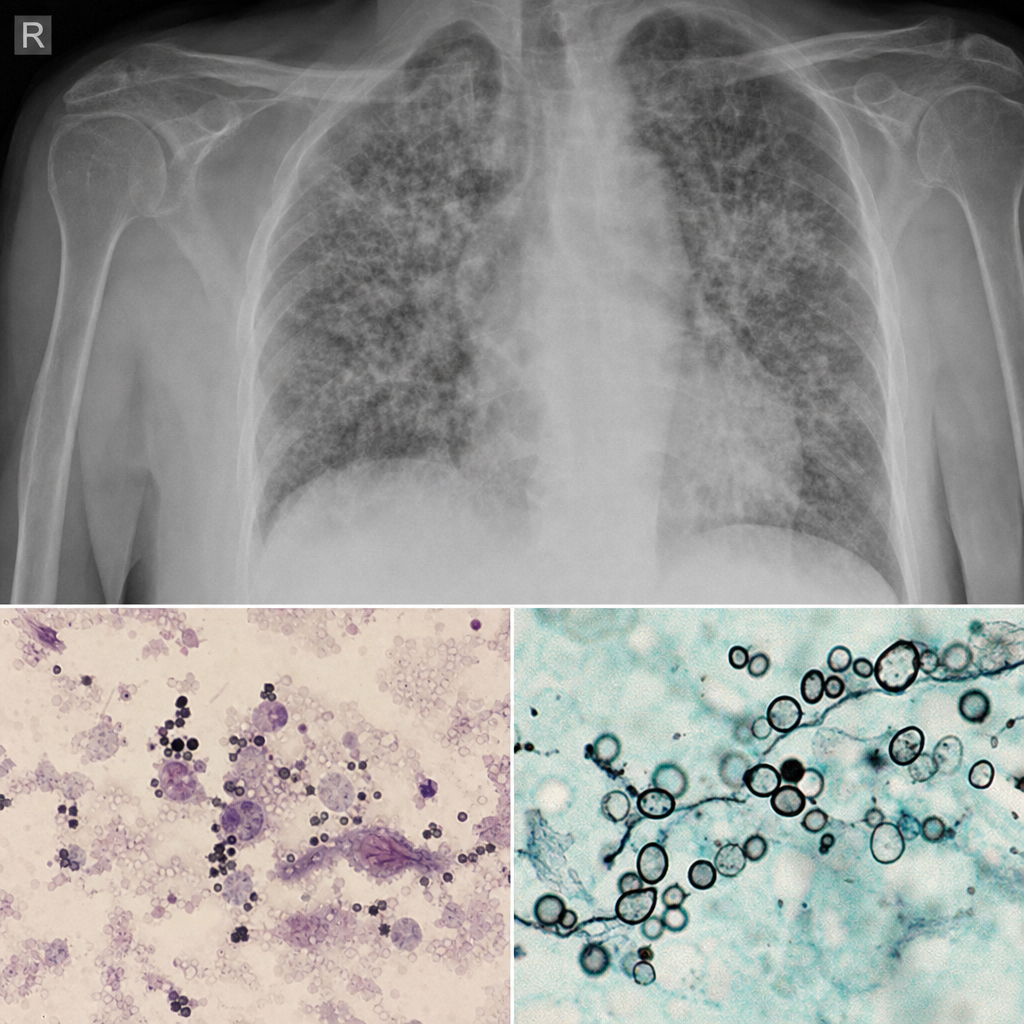
A 60-year-old female, known case of rheumatoid ahritis presented to the ER with shoness of breath, fever and cough for 2 days. Patient was staed on infliximab 2 months ago. On examination, Hypotension Hypoxemic Not maintaining spO2 on room air. Patient was diagnosed with respiratory failure and put on mechanical ventilation. Bronchioalveolar lavage was done and subjected to silver staining. Chest x-ray What is the most likely diagnosis in the above condition: -
Tinea versicolor is caused by:
Which one of the following diseases is endogenous in origin-
An 8-year-old male presents with multiple patches of alopecia and severe pruritus. A bright blue-green fluorescence is seen on examination of the scalp with a Wood's lamp. Pathogen most likely responsible is?
Which of the following is most likely to be acquired by traumatic inoculation?
Which is not a dimorphic fungus?
Practice by Chapter
Classification of Fungi
Practice Questions
Superficial Mycoses
Practice Questions
Dermatophytes
Practice Questions
Subcutaneous Mycoses
Practice Questions
Candidiasis
Practice Questions
Aspergillosis
Practice Questions
Cryptococcosis
Practice Questions
Zygomycosis
Practice Questions
Endemic Mycoses
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Antifungal Agents
Practice Questions
Laboratory Diagnosis of Fungal Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app