
Mycology — MCQs

On this page
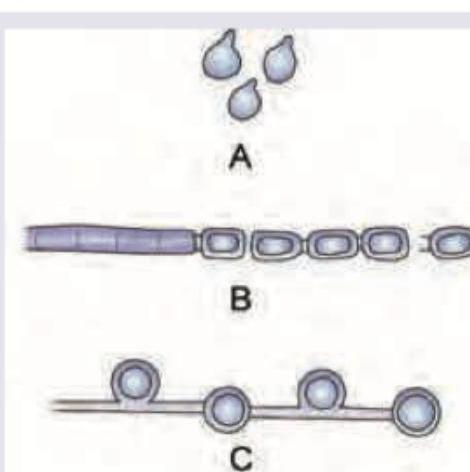
Which of the following is correct about the vegetative fungal spores?
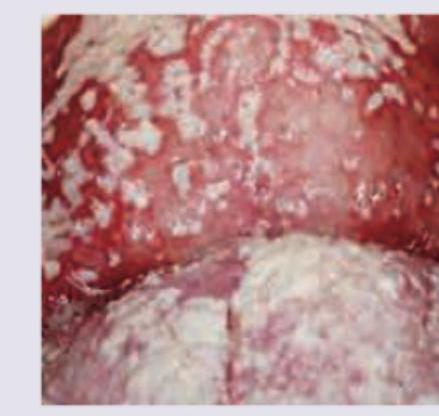
All are correct about the organism causing the following lesion except:
All are correct about the image shown except:
A patient walking barefoot during his morning walk has developed a chronic, painless, progressive swelling in the foot with draining sinuses and visible grains. What is the probable diagnosis?

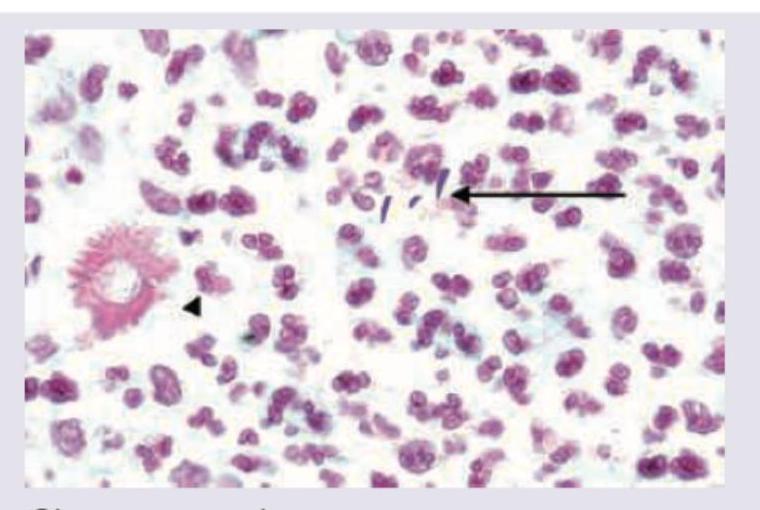
A carpenter presents with a nodule on dorsum of hand which ulcerates after few days and has not healed for last 2 months. Biopsy of lesion was performed and shown below. Diagnosis is:
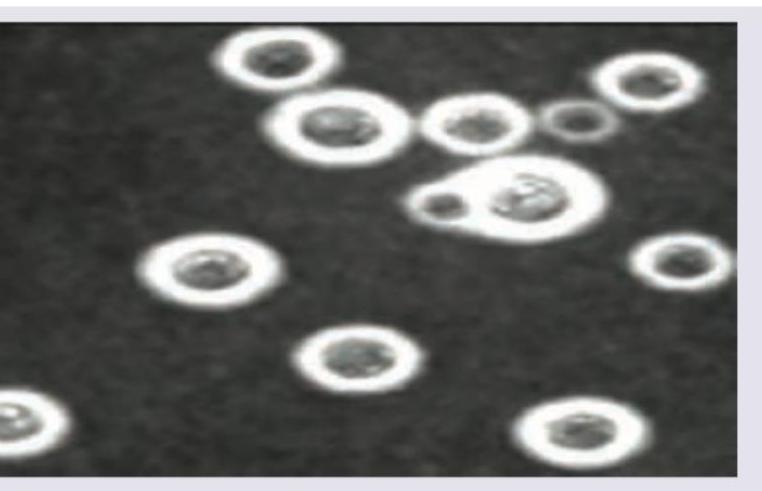
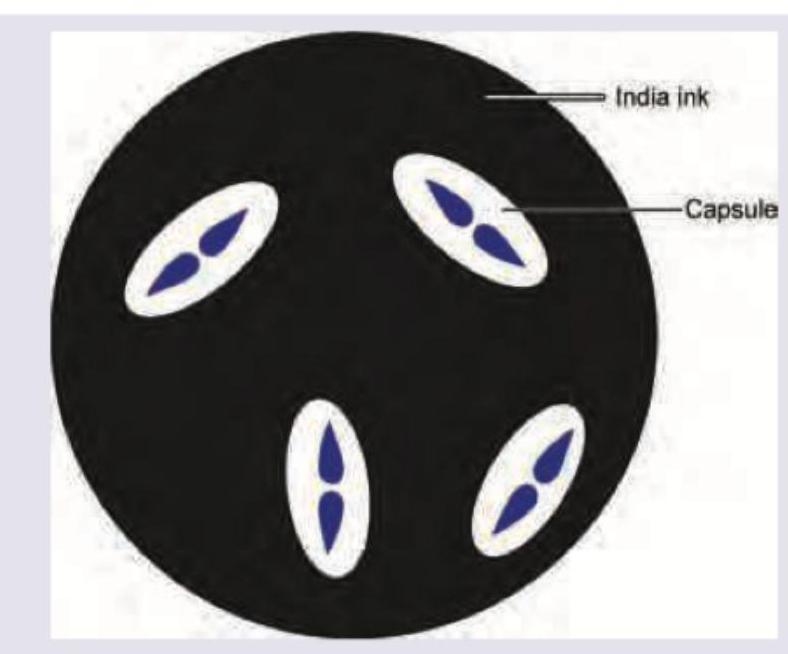
A 25-year-old truck driver presents with history of fever for 3 days with altered sensorium for 1 day. On the way to hospital he had an episode of vomiting followed by seizures. On examination reflexes are brisk and neck stiffness was noted. Mannitol was given and urgent brain imaging excluded a mass lesion or obstructive hydrocephalus before Lumbar puncture was performed. The microscopic examination of CSF sample yields the view given below. What is the diagnosis?
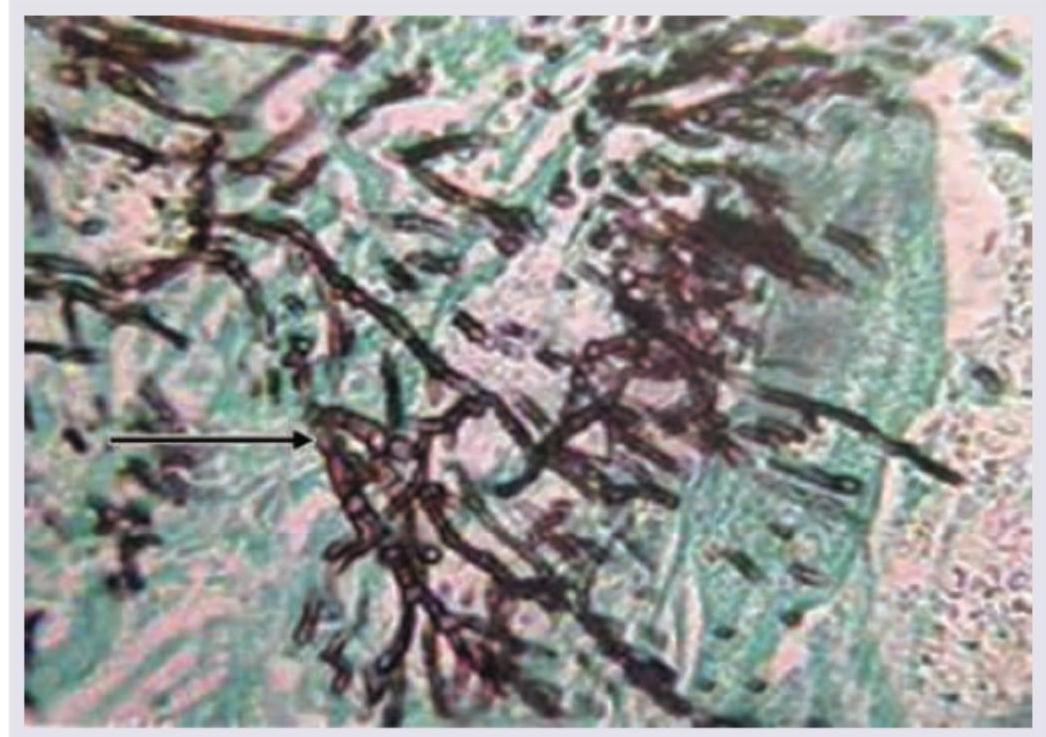
Identify the fungal organism in this slide stained with Gomori-methenamine silver stain. (AIIMS Nov 2017)
A young male presents with the following itchy lesion for one month. All of the following genera can cause this kind of lesion except:

The given KOH mount of a patient shows:
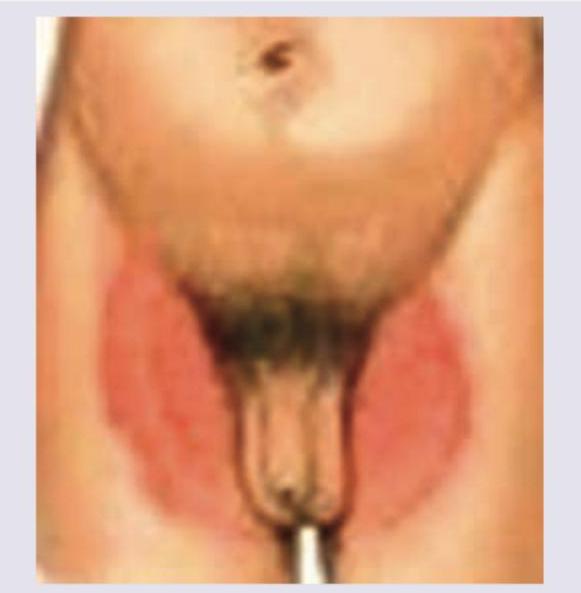
A patient has the following tinea cruris. Which of the following cannot be a cause?
Practice by Chapter
Classification of Fungi
Practice Questions
Superficial Mycoses
Practice Questions
Dermatophytes
Practice Questions
Subcutaneous Mycoses
Practice Questions
Candidiasis
Practice Questions
Aspergillosis
Practice Questions
Cryptococcosis
Practice Questions
Zygomycosis
Practice Questions
Endemic Mycoses
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Antifungal Agents
Practice Questions
Laboratory Diagnosis of Fungal Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app