
Mycology — MCQs

On this page
A 63-year-old man with insulin-dependent diabetes develops a black, crusting lesion in the nose and left maxillary sinus. Biopsy reveals nonseptate hyphae. What is the diagnosis?
Which of the following represents a dimorphic fungus causing subcutaneous mycosis?
Pneumocystis carinii typically infects which host?
Inhalation of fungal spores can cause primary lung infections. Which of the following organisms is most likely to be associated with this mode of transmission?
What is the causative agent of Favus?
Budding reproduction in tissue is seen in which of the following?
An AIDS-positive patient came with a history of fever, vomiting, and meningismus. Which of the following tests help in the rapid diagnosis of cryptococcal meningitis?
Identify the opportunistic pathogen demonstrating a 'crushed ping pong ball appearance' on Gomori methenamine stain shown in the image.
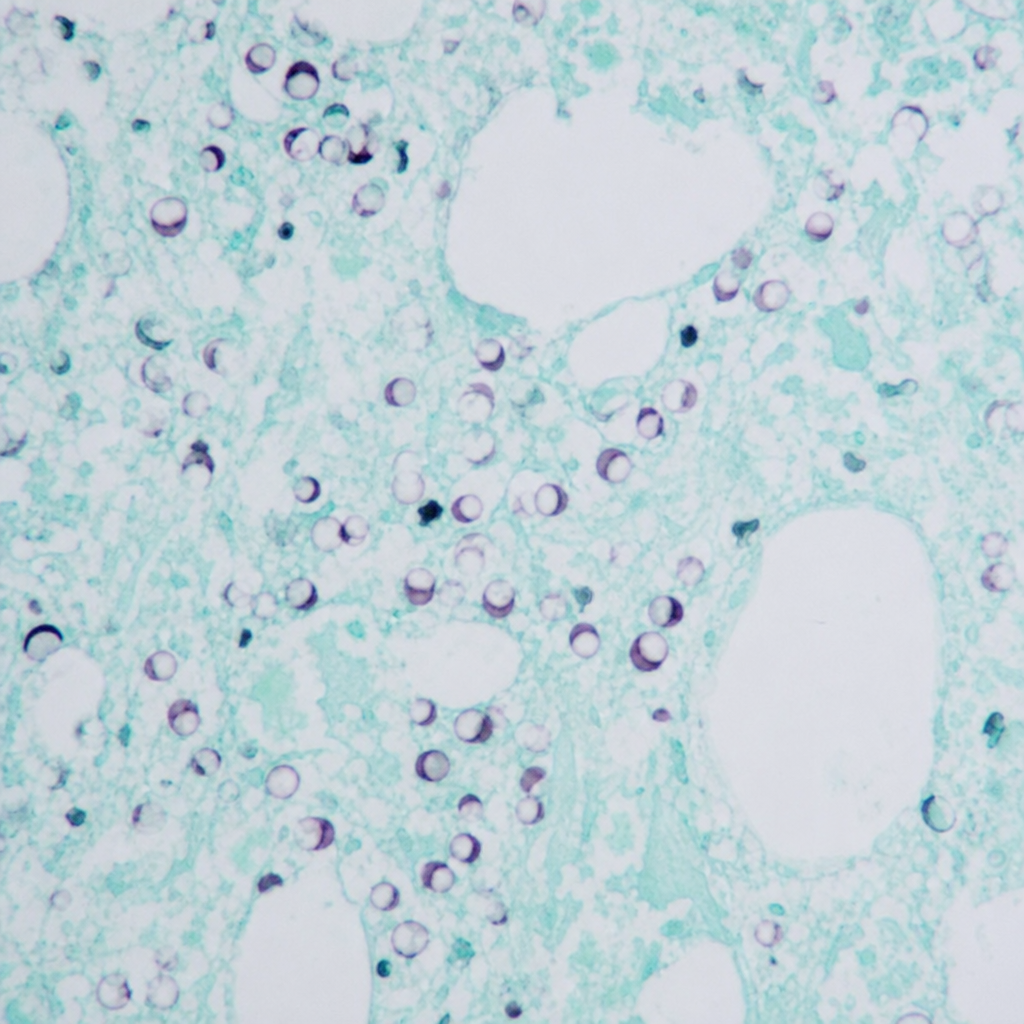
Which opportunistic pathogen demonstrates a “crushed ping pong ball appearance” on Gomori methenamine stain?
A person came with the H/o thorn prick a week ago. A few days later, he developed ulcers along lymphatic drainage. Choose the correct organism.
Practice by Chapter
Classification of Fungi
Practice Questions
Superficial Mycoses
Practice Questions
Dermatophytes
Practice Questions
Subcutaneous Mycoses
Practice Questions
Candidiasis
Practice Questions
Aspergillosis
Practice Questions
Cryptococcosis
Practice Questions
Zygomycosis
Practice Questions
Endemic Mycoses
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Antifungal Agents
Practice Questions
Laboratory Diagnosis of Fungal Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app