
Mycology — MCQs

On this page
Draining sinuses are seen in which of the following conditions?
A patient with a previous history of tuberculosis complains of hemoptysis. Chest x-ray reveals an upper lobe mass with a cavity and a crescent-shaped air-fluid level. What is the most likely etiologic agent?
In an AIDS patient presenting with fever and cough, a diagnosis of Pneumocystis jirovecii pneumonia is best established by?
Barrel-shaped spores are seen with which of the following fungi?
A 40-year-old male presents with verrucous skin lesions. Microscopic examination of a tissue biopsy shows characteristic findings. What is the diagnosis?
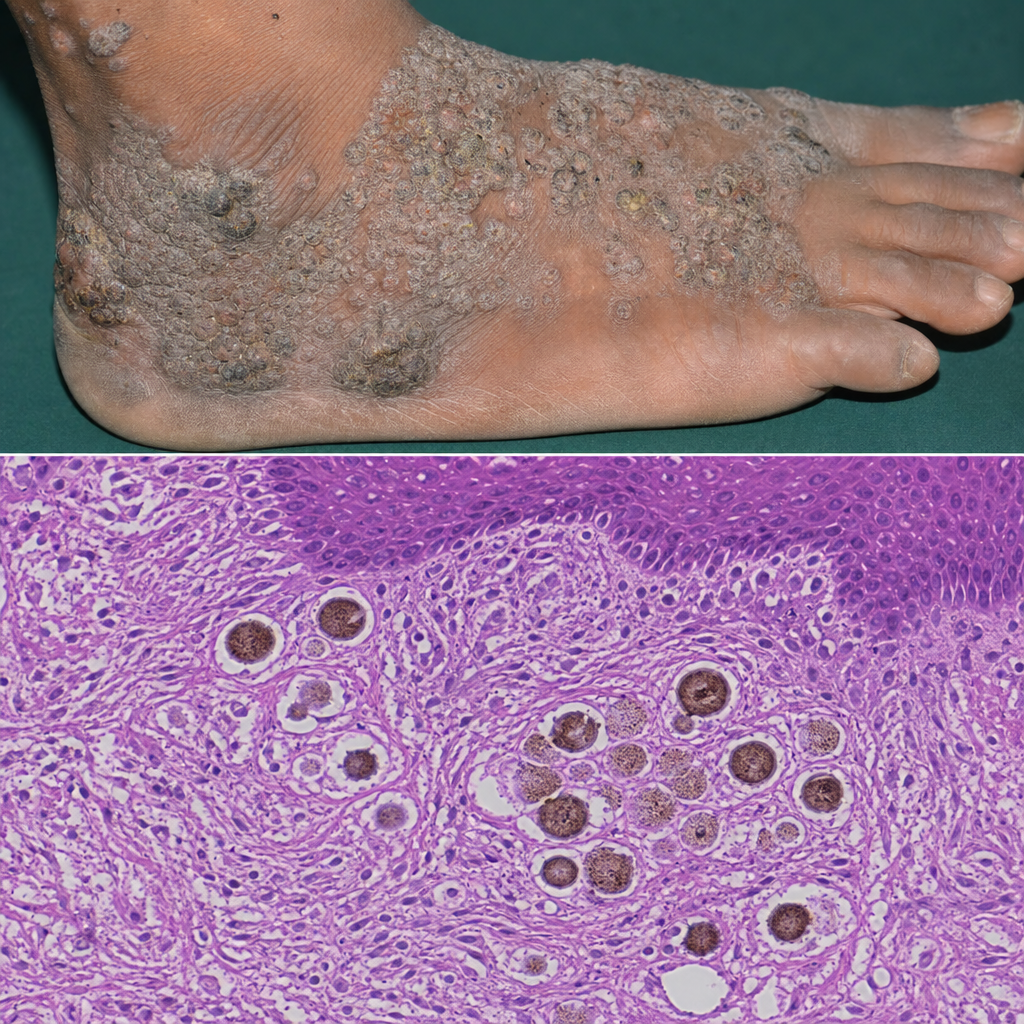
A patient presents with foot swelling, pus discharge, and multiple sinuses. A KOH smear reveals filamentous structures. What is the most likely diagnosis?
Orbital mucormycosis is a complication of -
Which of the following is NOT true about Cryptococcus?
An AIDS patient with clinical pneumonia has a bronchoalveolar lavage that demonstrates small, "hat-shaped" structures in alveoli that are about the size of an erythrocyte and stain with silver stains. The microorganism involved is most likely which of the following?
Prolonged use of antibiotics in children can result in which of the following conditions?
Practice by Chapter
Classification of Fungi
Practice Questions
Superficial Mycoses
Practice Questions
Dermatophytes
Practice Questions
Subcutaneous Mycoses
Practice Questions
Candidiasis
Practice Questions
Aspergillosis
Practice Questions
Cryptococcosis
Practice Questions
Zygomycosis
Practice Questions
Endemic Mycoses
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Antifungal Agents
Practice Questions
Laboratory Diagnosis of Fungal Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app