
Mycology — MCQs

On this page
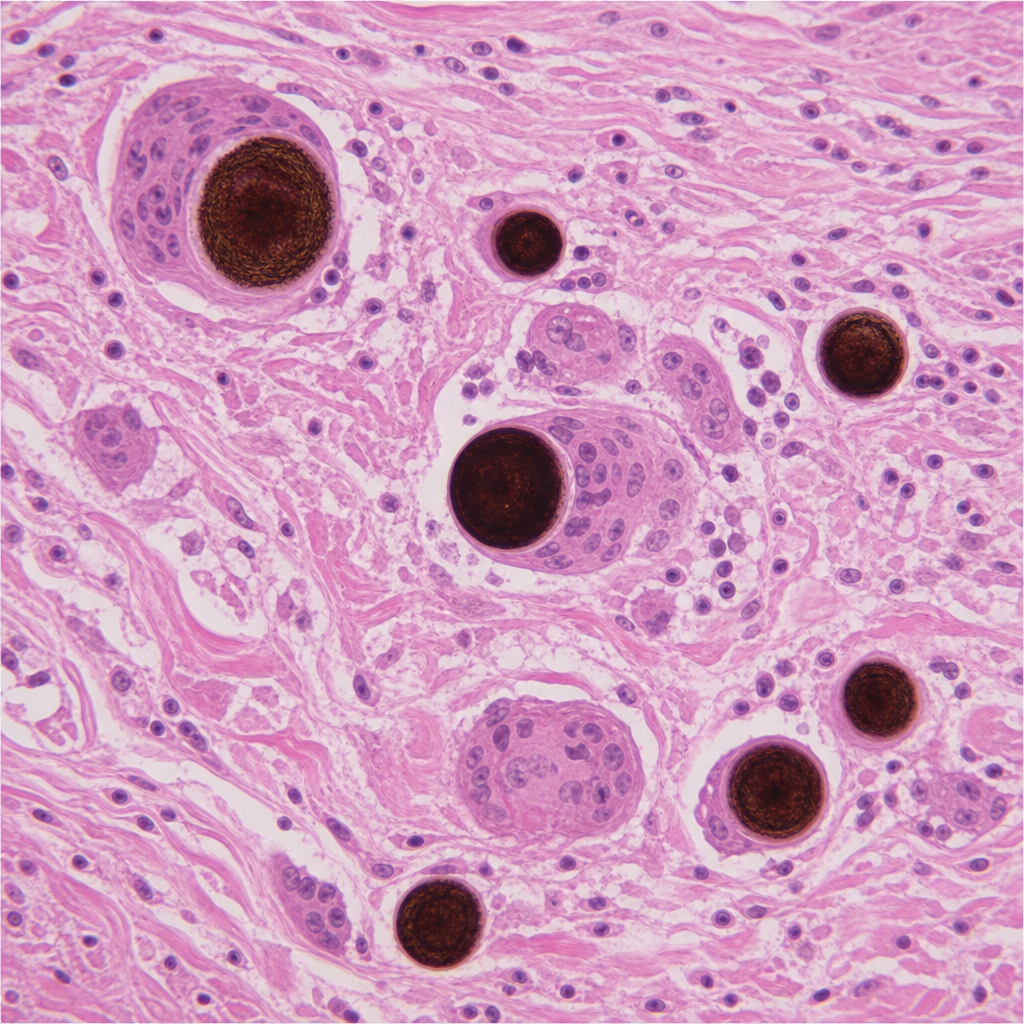
Melanized sclerotic cells / Medlar bodies (4-12 µm diameter) evident in this H & E stained cutaneous biopsy are characteristic of which disease?
Which of the following statements about Cryptococcus is FALSE?
Which of the following statements regarding Candida is true?
A patient with severe mycotic infection, diabetes mellitus, and cellulitis is suffering from which condition?
Which of the following is the rarest opportunistic fungal infection seen in an AIDS patient?
A patient presented with a swelling in his right foot with multiple discharging sinuses that contained brown granules. The lesion did not respond to antibiotic medications. Which of the following is the causative agent?
Which of the following statements is true regarding Cryptococcus neoformans?
A diabetic patient presents with bloody nasal discharge, orbital swelling, and pain. The culture of periorbital pus shows branching septate hyphae. Which of the following is the most probable organism involved?
A diabetic patient presents with orbital cellulitis and maxillary sinusitis. Microscopy shows a fungus with hyaline, narrow septate, and branching hyphae that invades blood vessels. Which is the causative fungus?
Which organism produces black-coloured grains in mycetoma?
Practice by Chapter
Classification of Fungi
Practice Questions
Superficial Mycoses
Practice Questions
Dermatophytes
Practice Questions
Subcutaneous Mycoses
Practice Questions
Candidiasis
Practice Questions
Aspergillosis
Practice Questions
Cryptococcosis
Practice Questions
Zygomycosis
Practice Questions
Endemic Mycoses
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Antifungal Agents
Practice Questions
Laboratory Diagnosis of Fungal Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app