
Mycology — MCQs

On this page
Which of the following organisms is most likely responsible for this finding?
A diabetic patient presents with facial pain, black nasal eschar and eye pain following corticosteroid therapy. What is the etiological agent?
A patient presents with fever, headache, and neck stiffness suggestive of meningitis. CSF examination is performed, and Nigrosin stain reveals encapsulated budding yeast cells. Which of the following organisms is the most likely causative agent?
Which statement is false regarding Cryptococcus neoformans?
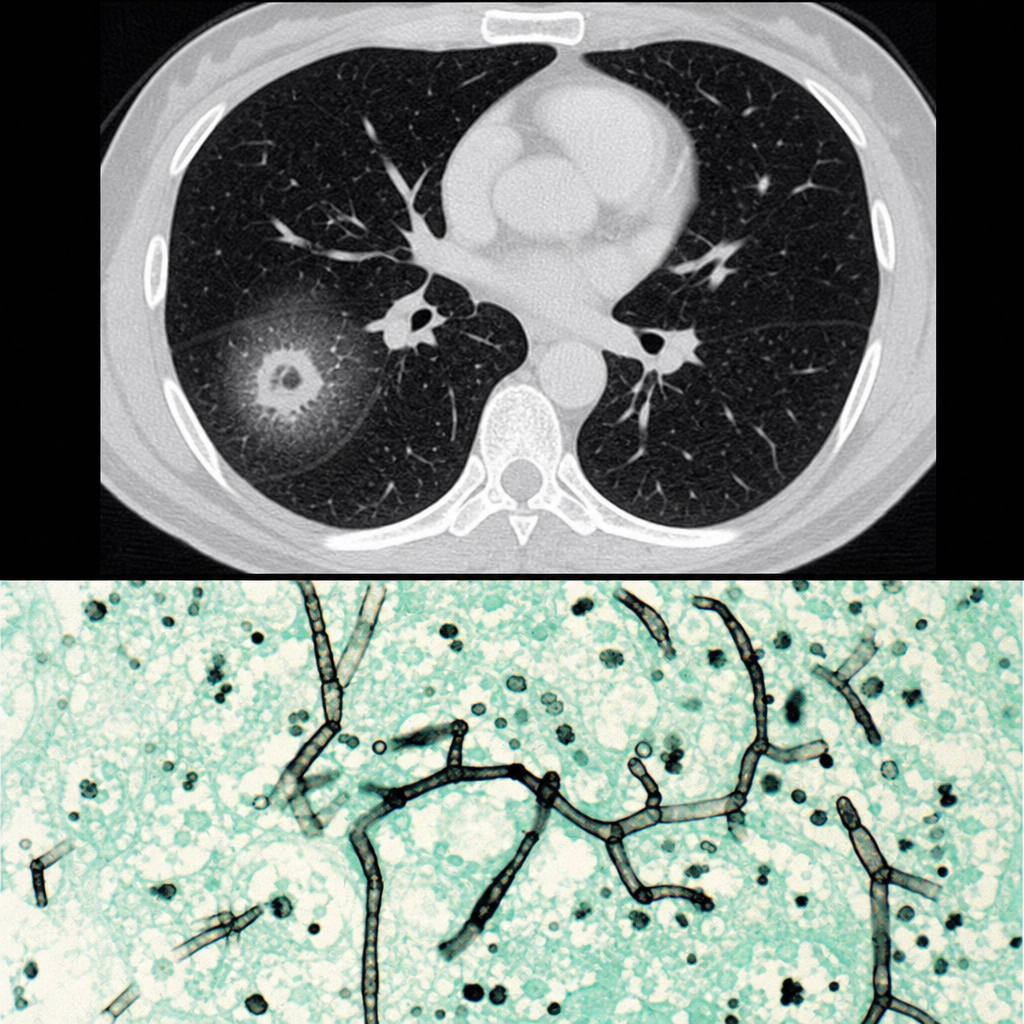
About 90 days post-bone marrow transplant, a 55-year-old white woman began to complain of dry cough, shortness of breath, and chest pain. She was started on antibiotics and blood culture obtained at the time was negative and there was not improvement. A computed tomography (CT) scan of the lungs showed a halo of low attenuation around a nodular lesion. Analysis of lung biopsy was similar to methenamine silver-stained section below. What is the most likely diagnosis for this patient?
Brown, spherical, septate bodies found in pus are diagnostic of which condition?
San Joaquin Valley fever is caused by which organism?
Opportunistic lung infections in AIDS are most commonly caused by which of the following pathogens?
Gram stained periorbital exudates in severe panophthalmitis with cellulitis in an elderly diabetic shows irregular branching aseptate and broad hyphae. Which of the following is the most likely diagnosis?
Maltese cross formation is observed on polarizing microscopy in which of the following?
Practice by Chapter
Classification of Fungi
Practice Questions
Superficial Mycoses
Practice Questions
Dermatophytes
Practice Questions
Subcutaneous Mycoses
Practice Questions
Candidiasis
Practice Questions
Aspergillosis
Practice Questions
Cryptococcosis
Practice Questions
Zygomycosis
Practice Questions
Endemic Mycoses
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Antifungal Agents
Practice Questions
Laboratory Diagnosis of Fungal Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app