
Microbial Genetics — MCQs

On this page
The following image shows:
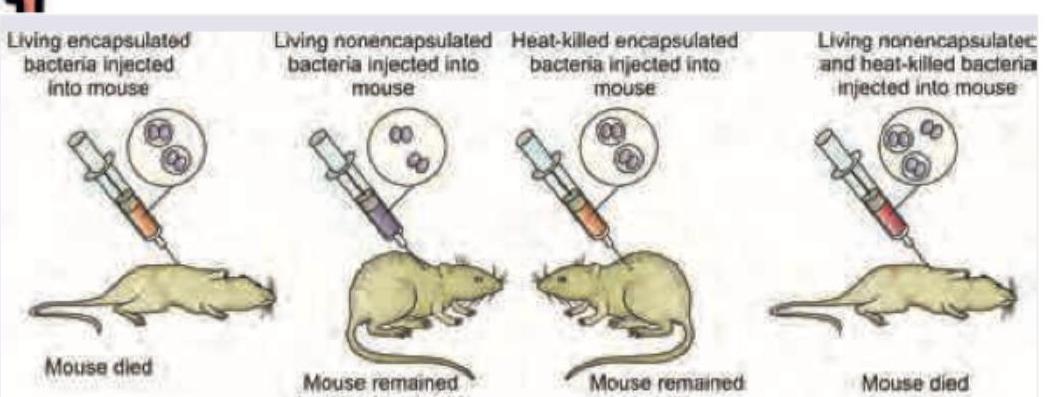
The following image shows:

DNA transfer in bacteria by phage is:
What is the mode of transmission of genetic material to bacteria through bacteriophage?
Which statement concerning plasmids is true?
False regarding bacterial plasmids is:
F factor integrates with bacterial chromosome to form -
The mechanism of direct transfer of free DNA involves _____
Which of the following organisms is a natural transformer?
All the following terms are used to describe bacterial chromosome Except
Practice by Chapter
Bacterial Genome Organization
Practice Questions
Plasmids and Mobile Genetic Elements
Practice Questions
Bacterial Gene Expression
Practice Questions
Mutation and Mutagenesis
Practice Questions
Gene Transfer in Bacteria
Practice Questions
Transposons and Insertion Sequences
Practice Questions
Bacterial Genetic Recombination
Practice Questions
Regulation of Gene Expression
Practice Questions
CRISPR-Cas Systems
Practice Questions
Bacterial Stress Responses
Practice Questions
Genetics of Antimicrobial Resistance
Practice Questions
Genetic Basis of Bacterial Virulence
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app