
Infectious Diseases — MCQs

On this page
Frie's test is useful for the diagnosis of which condition?
Which of the following is a true statement regarding the Widal test in typhoid fever?
A 32-year-old person presents to the hospital with a 2-week history of diarrhea. Which of the following investigations can confirm the diagnosis of typhoid fever?
Which of the following infections is NOT transmitted through blood transfusion?
Which of the following statements regarding the transmission of infectious agents is NOT true?
Typhoid fever in the first week of illness is best diagnosed by?
A false positive VDRL test is seen in all of the following conditions except?
What reaction is due to lysis of bacterial cell wall and necrotic cell products?
Which among the following causes Malta fever?
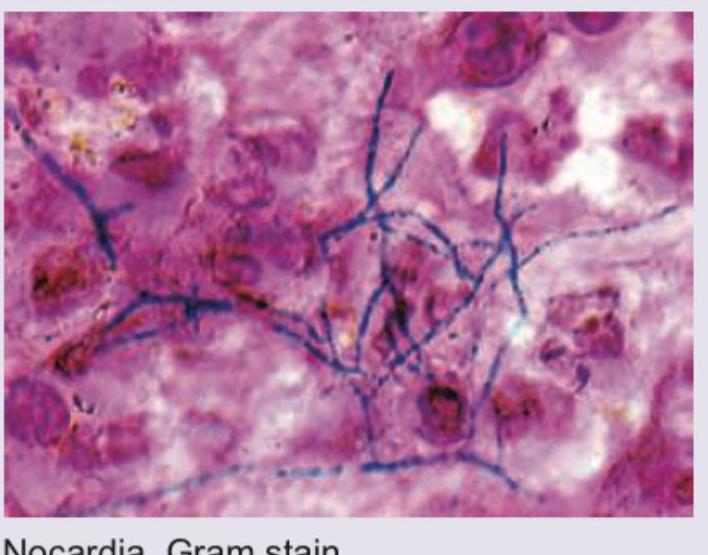
Stereotactic CT based aspiration from a patient with brain abscess was performed. Identify the organism seen and the stain used.
Practice by Chapter
Respiratory Tract Infections
Practice Questions
Urinary Tract Infections
Practice Questions
Gastrointestinal Infections
Practice Questions
Skin and Soft Tissue Infections
Practice Questions
Central Nervous System Infections
Practice Questions
Bone and Joint Infections
Practice Questions
Cardiovascular Infections
Practice Questions
Sexually Transmitted Infections
Practice Questions
Zoonotic Infections
Practice Questions
Bloodstream Infections and Sepsis
Practice Questions
Fever of Unknown Origin
Practice Questions
Infections in Immunocompromised Host
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app