
Infectious Diseases — MCQs

On this page
A patient presents with a painless genital ulcer followed by painful inguinal buboes (lymphadenopathy). Which strains of Chlamydia trachomatis are responsible for this condition?
A female presents with high grade fever, diffuse erythematous rash and hypotension. She is currently menstruating and using tampoons. The toxin responsible acts by?
A 32-year-old woman with a history of splenectomy presents to the emergency department with sudden-onset high-grade fever, vomiting, hypotension, and rapidly progressive septic shock. Her symptoms began 2 weeks after a minor febrile illness. Which organism is the most likely causative agent of this life-threatening condition?
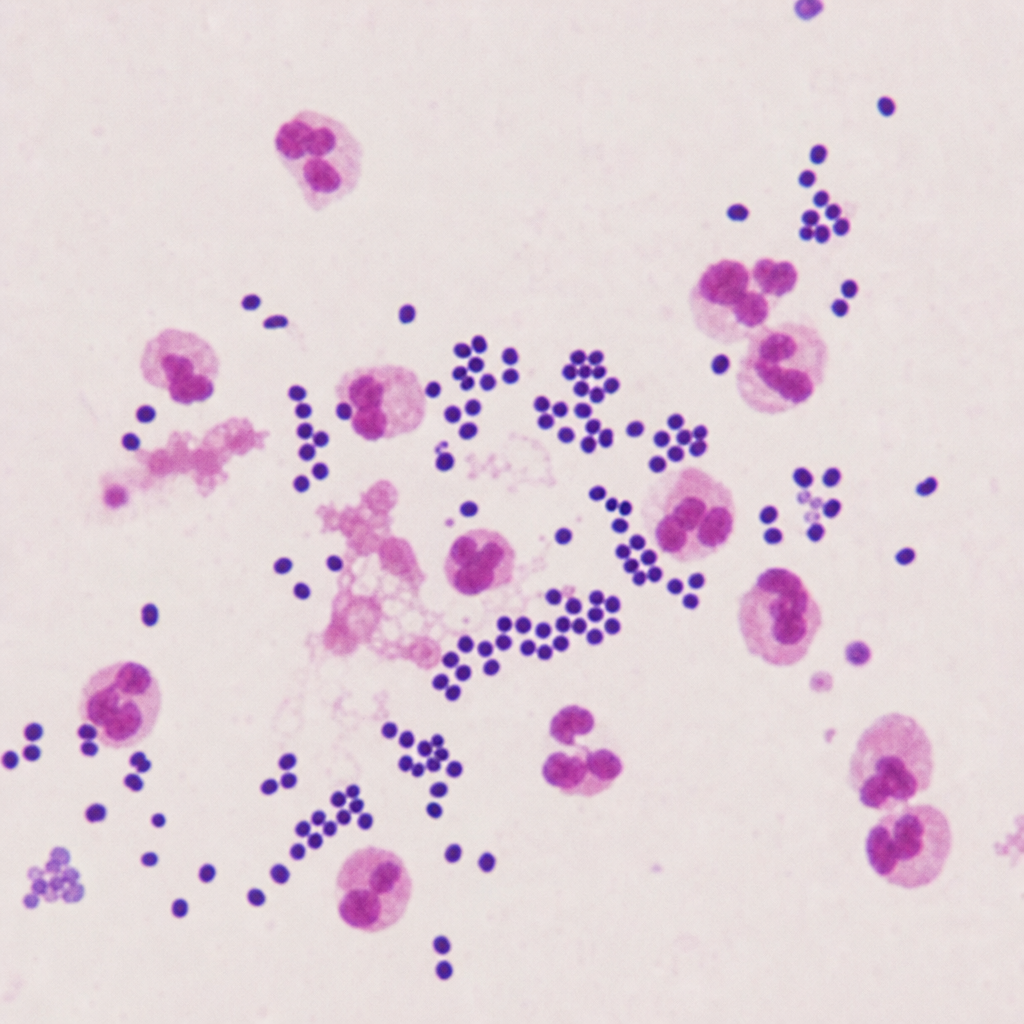
A 34-year-old man with a CD4 count of 48 cells/µL presents with a 3-week history of progressive headache, low-grade fever, and neck stiffness. Lumbar puncture reveals elevated opening pressure, low glucose, and elevated protein. CSF microscopy is shown (Image 1). Which of the following best describes the virulence mechanism of the organism identified that directly enables its evasion of phagocytic killing in the host?
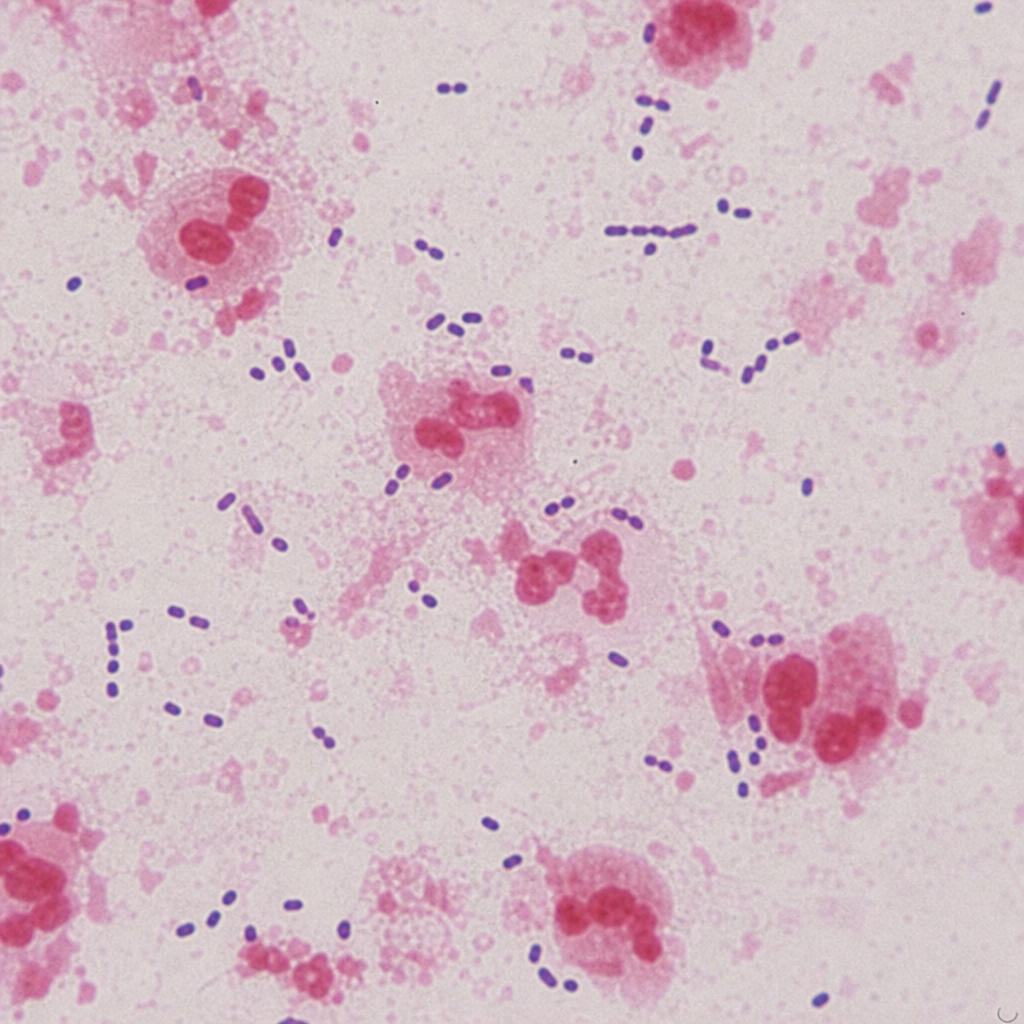
A 65-year-old diabetic male presents with high-grade fever, productive rust-coloured sputum, and right-sided pleuritic chest pain for 3 days. His oxygen saturation is 88% on room air. A sputum Gram stain is performed (Image 1). Which of the following tests would most definitively confirm the identity of this organism from a positive blood culture?
Practice by Chapter
Respiratory Tract Infections
Practice Questions
Urinary Tract Infections
Practice Questions
Gastrointestinal Infections
Practice Questions
Skin and Soft Tissue Infections
Practice Questions
Central Nervous System Infections
Practice Questions
Bone and Joint Infections
Practice Questions
Cardiovascular Infections
Practice Questions
Sexually Transmitted Infections
Practice Questions
Zoonotic Infections
Practice Questions
Bloodstream Infections and Sepsis
Practice Questions
Fever of Unknown Origin
Practice Questions
Infections in Immunocompromised Host
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app