
Immunology — MCQs

On this page
Activation of naïve B lymphocytes by protein antigens is?
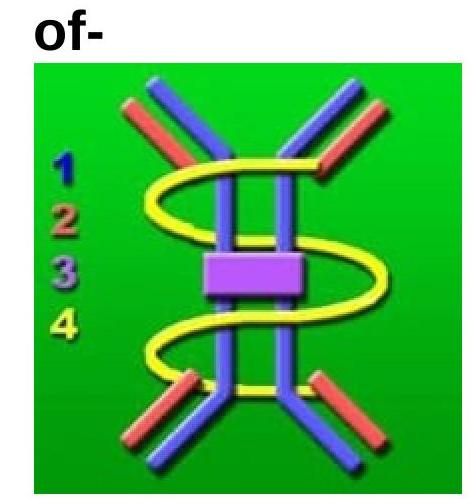
The image of an immunoglobulin is shown below. Which type of immunoglobulin is it?
Which interleukin is primarily responsible for inducing IgE production from B cells?
Which antibody is not transmitted from mother to baby?
Which protein is produced by B lymphocytes and not synthesized in the liver?
What is required for precipitation in comparison to agglutination?
Haptens are immunogenic when they covalently bind to which type of carrier?
Which human IgG subclass has the highest serum concentration?
Which of the following does not stimulate active immunity?
To which part of an antigen do monoclonal antibodies specifically bind?
Practice by Chapter
Cells and Organs of Immune System
Practice Questions
Innate Immunity
Practice Questions
Adaptive Immunity
Practice Questions
Antigens and Antibodies
Practice Questions
Major Histocompatibility Complex
Practice Questions
Complement System
Practice Questions
Cytokines and Chemokines
Practice Questions
Hypersensitivity Reactions
Practice Questions
Autoimmunity and Autoimmune Diseases
Practice Questions
Immunodeficiency Disorders
Practice Questions
Transplantation Immunology
Practice Questions
Tumor Immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app