
Immunology — MCQs

On this page
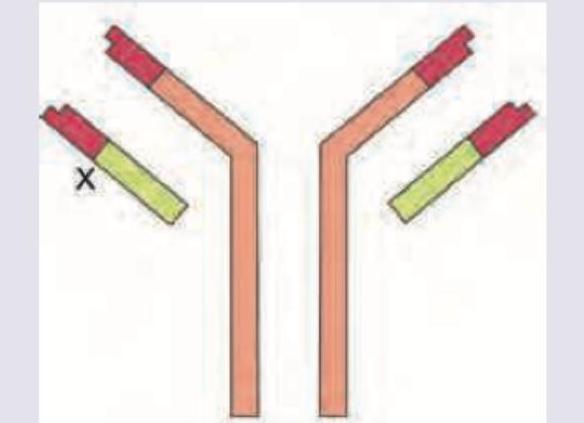
Identify the antibody shown in the diagram which has a joining chain and is mainly found in mucosal areas.
A patient presents with recurrent infections with Neisseria gonorrhoeae. Which of the following investigations is most appropriate to evaluate the underlying immunodeficiency?
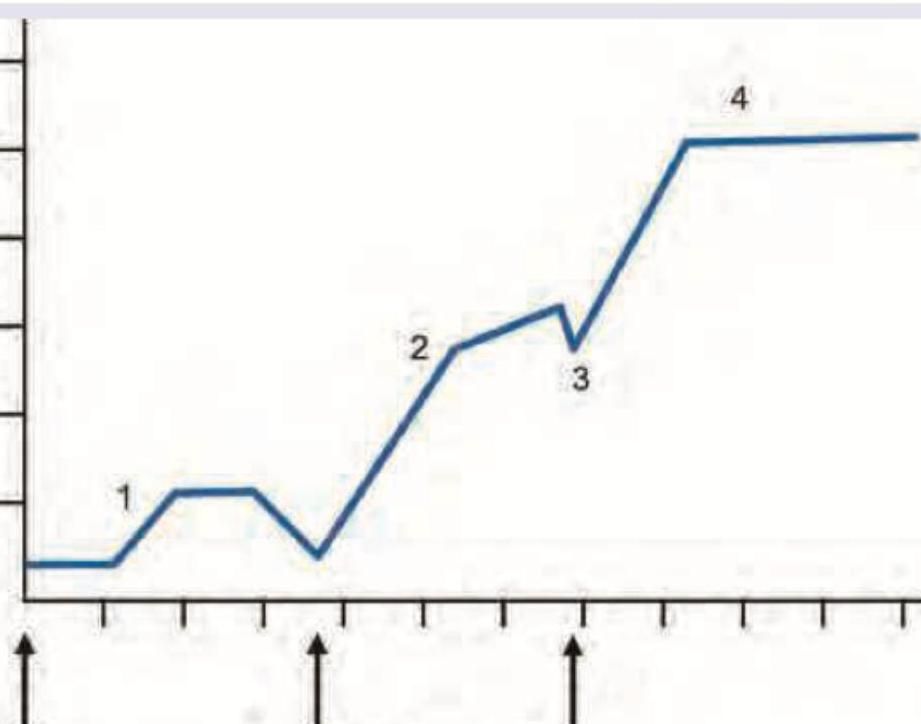
The following image shows effect of repeated antigenic stimulus on antibody production. What does phase 3 represent?
All are correct about the **X** mark in antibody structure except: (Recent NEET Pattern 2016-17)
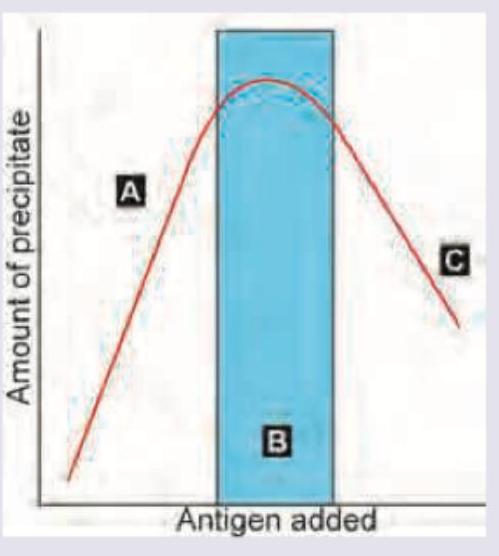
Which of the following is correct about the picture shown?
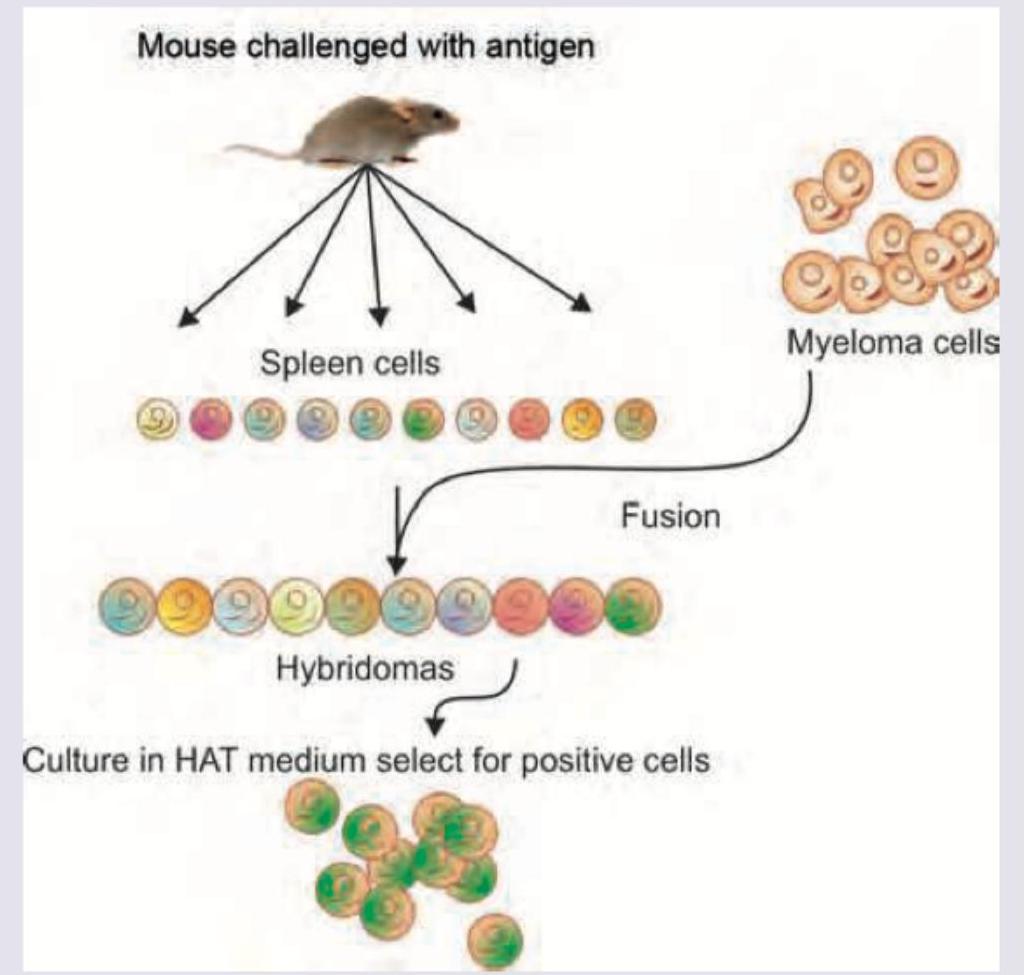
The technique shown in the picture is used for: (AIIMS Nov 2018)
Which one of the following statements about Human Immunoglobulins is not correct?
During the EARLY phase of a primary immune response, which of the following best describes the relationship between peak IgM and IgG antibody levels?
Antigen presented on MHC class I molecules activates which of the following cells?
Affinity maturation of antibodies is because of _____ .
Practice by Chapter
Cells and Organs of Immune System
Practice Questions
Innate Immunity
Practice Questions
Adaptive Immunity
Practice Questions
Antigens and Antibodies
Practice Questions
Major Histocompatibility Complex
Practice Questions
Complement System
Practice Questions
Cytokines and Chemokines
Practice Questions
Hypersensitivity Reactions
Practice Questions
Autoimmunity and Autoimmune Diseases
Practice Questions
Immunodeficiency Disorders
Practice Questions
Transplantation Immunology
Practice Questions
Tumor Immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app