
Immunology — MCQs

On this page
Which Toll-like receptor is associated with viruses?
In which of the following conditions is the prozone phenomenon most evident?
Which of the following conditions represents a disorder of T-cell function?
At what age does the capacity for producing IgG develop?
Which of the following statements regarding agglutination reaction is NOT true?
A patient presents with recurrent swelling of the lips. He has no itching and a positive family history. Which of the following is deficient in this patient?
Division and differentiation of B cells leading to production of plasma cells both require:
Which of the following statements best applies to the given diagram?
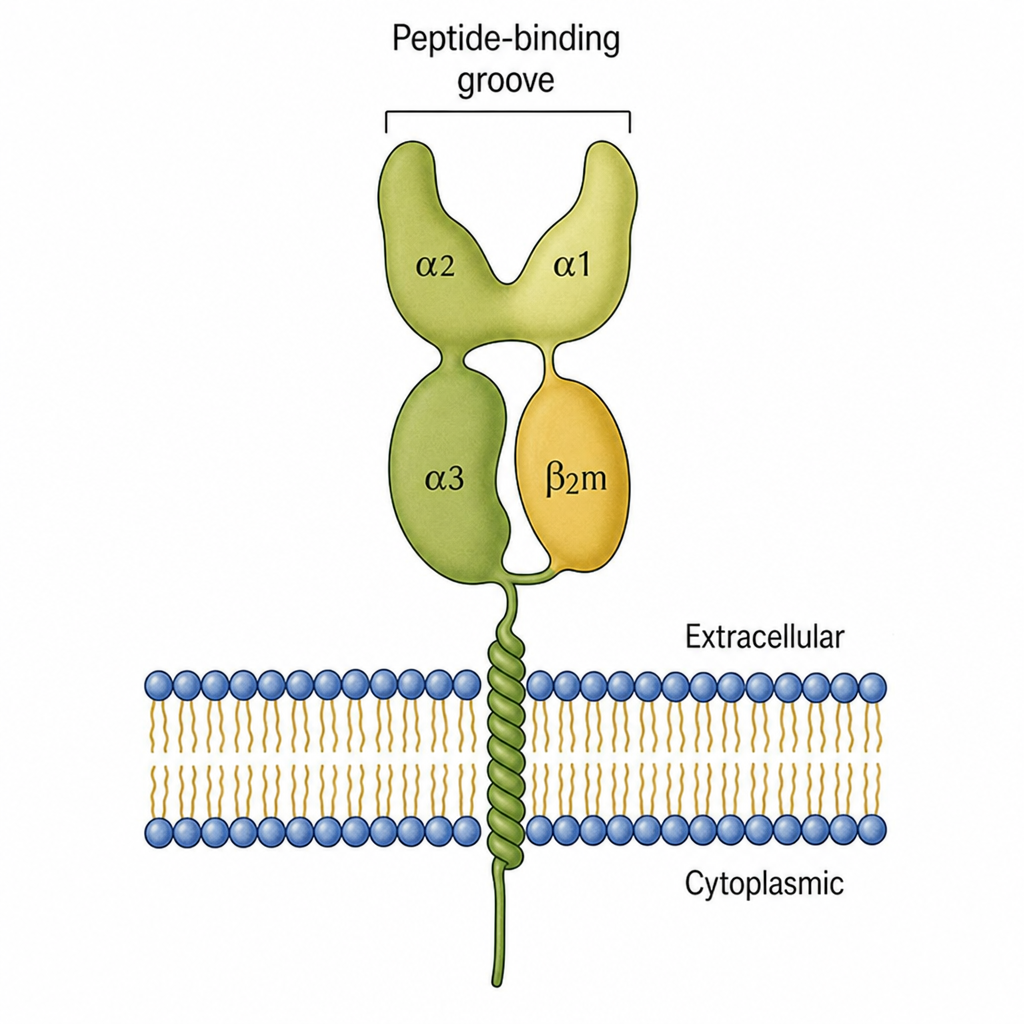
Antigens processed by the exogenous antigen presentation pathway are presented in association with which of the following?
What is the earliest immunoglobulin synthesized by the fetus?
Practice by Chapter
Cells and Organs of Immune System
Practice Questions
Innate Immunity
Practice Questions
Adaptive Immunity
Practice Questions
Antigens and Antibodies
Practice Questions
Major Histocompatibility Complex
Practice Questions
Complement System
Practice Questions
Cytokines and Chemokines
Practice Questions
Hypersensitivity Reactions
Practice Questions
Autoimmunity and Autoimmune Diseases
Practice Questions
Immunodeficiency Disorders
Practice Questions
Transplantation Immunology
Practice Questions
Tumor Immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app