
Cytokines and Chemokines — MCQs

The acute inflammatory response is predominantly mediated by which type of immune cells?
Which of the following is not classified as a chemokine?
Which of the following is the platinum-based chemotherapeutic agent used as first-line treatment for ovarian carcinoma?
Which is NOT a feature of chronic inflammation?
Which interleukin is specifically secreted by Th17 cells?
TNF and IL-1 are produced by
Which interleukin is primarily responsible for inducing IgE production from B cells?
What is the primary effect of superantigens on T-cells?
Which of the following is the most potent stimulator of Naive T-cells?
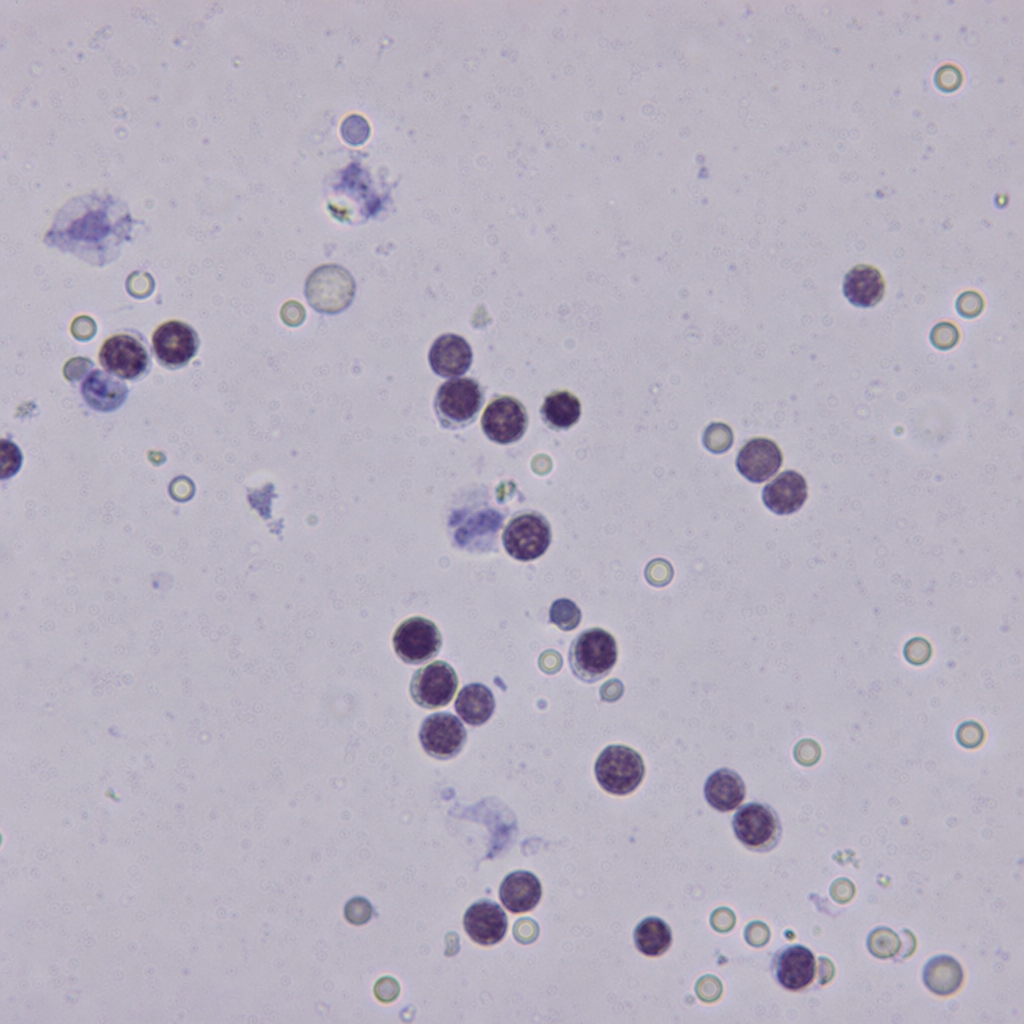
A 28-year-old male known to be HIV-positive with a CD4 count of 45 cells/µL presents with 2 weeks of progressive headache, photophobia, and neck stiffness. CSF opening pressure is markedly elevated. CSF microscopy is shown (Image 2). Which of the following statements most accurately describes the virulence mechanism that directly accounts for the markedly elevated CSF opening pressure seen in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app