
Immunology — MCQs

On this page
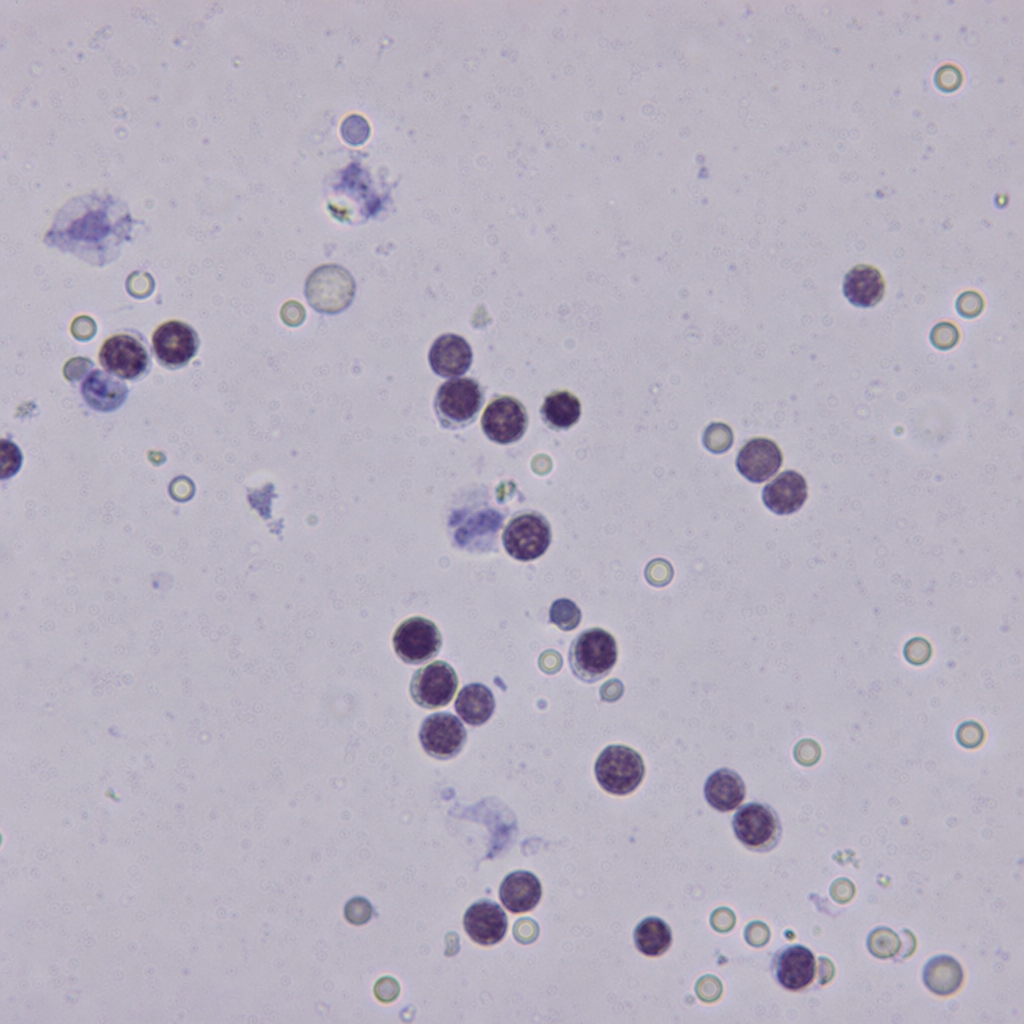
A 28-year-old male known to be HIV-positive with a CD4 count of 45 cells/µL presents with 2 weeks of progressive headache, photophobia, and neck stiffness. CSF opening pressure is markedly elevated. CSF microscopy is shown (Image 2). Which of the following statements most accurately describes the virulence mechanism that directly accounts for the markedly elevated CSF opening pressure seen in this patient?
Which of the following is true regarding lattice formation?
Which of the following is not encoded by the MHC Class III region?
What is the predominant immunoglobulin found in saliva?
Neisseria infections are associated with which of the following?
Practice by Chapter
Cells and Organs of Immune System
Practice Questions
Innate Immunity
Practice Questions
Adaptive Immunity
Practice Questions
Antigens and Antibodies
Practice Questions
Major Histocompatibility Complex
Practice Questions
Complement System
Practice Questions
Cytokines and Chemokines
Practice Questions
Hypersensitivity Reactions
Practice Questions
Autoimmunity and Autoimmune Diseases
Practice Questions
Immunodeficiency Disorders
Practice Questions
Transplantation Immunology
Practice Questions
Tumor Immunology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app