
Toxicology and Overdose Management — MCQs

On this page
A 20-year-old fireman presents with headache and dizziness after extinguishing a garage fire. He denies shortness of breath, and his arterial blood gas shows a normal PO2. There is no cyanosis. What is the best initial management step for this patient?
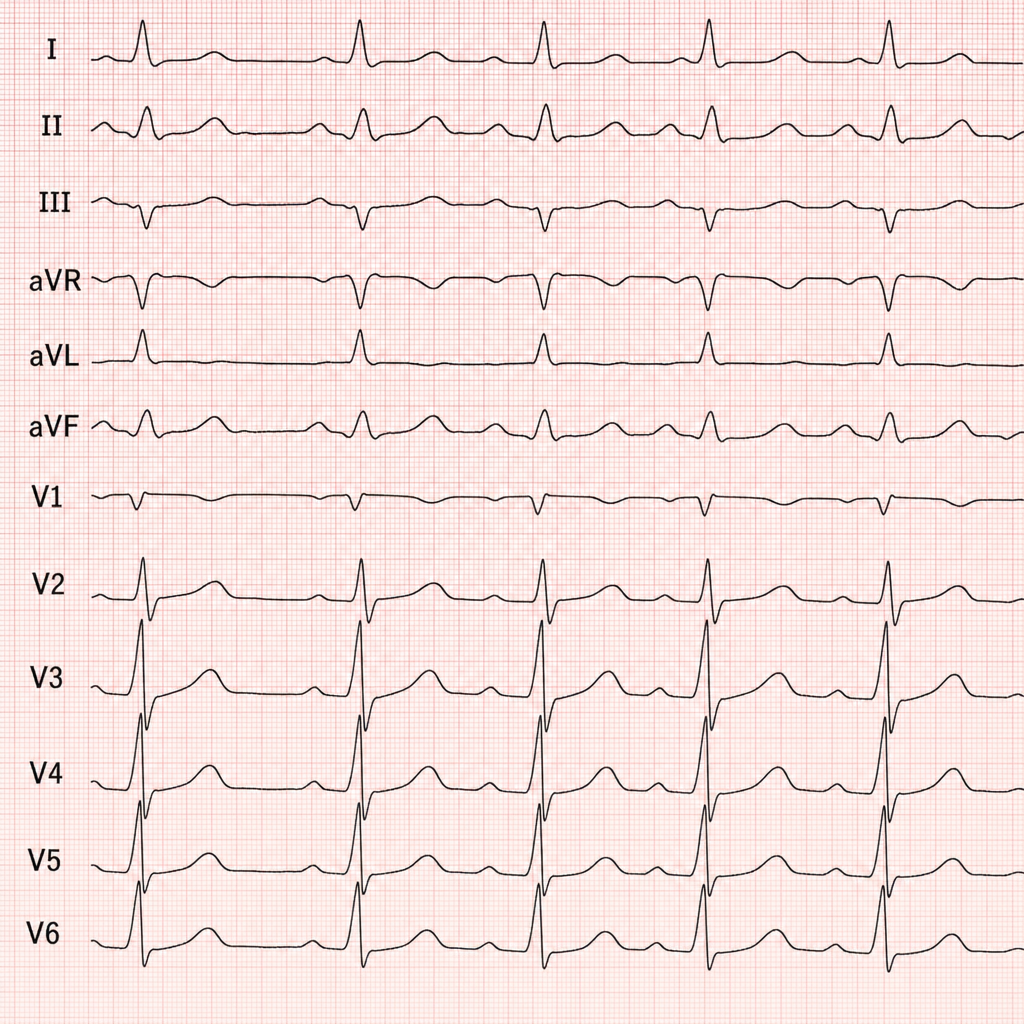
The ECG shows bidirectional ventricular tachycardia. Which of the following is the cause of this condition?
Heavy metal poisoning from mercury affects which part of the renal tubule?
A 50-year-old man is brought to the emergency department by ambulance. His respirations are shallow and infrequent, his pupils are constricted, and he is stuporous. He was noted to have suffered a grand mal seizure in the ambulance. Which drug is this man likely to have overdosed on?
What is the management for a 10-year-old girl presenting with acute paracetamol overdose?
A 27-year-old, previously healthy man suddenly collapses at a party where both legal and illicit drugs are being used. En route to the hospital, he requires resuscitation with defibrillation to establish a normal cardiac rhythm. On physical examination, his temperature is 40°C; respirations, 30/min; heart rate, 110/min; and blood pressure, 175/90 mm Hg. He has dilated pupils, a perforated nasal septum, and a prominent callus on the right thumb. CT scan of the head shows an acute right frontal lobe hemorrhage. Which of the following substances is most likely responsible for these findings?
In organophosphorus compound poisoning, atropine can reverse all the following signs except?
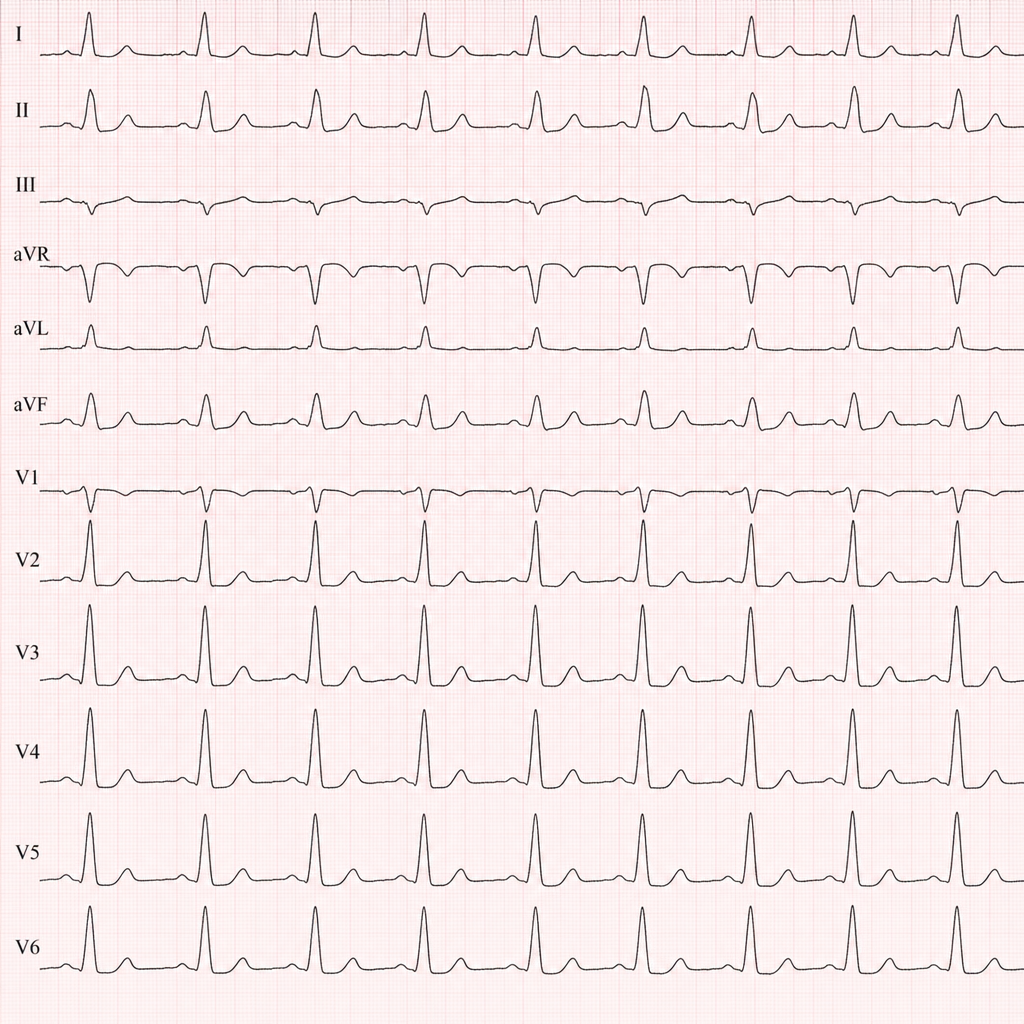
An ECG of a patient with snake bite is shown below. What is the abnormality seen?
A rubber industry worker presents with abdominal colic and severe anemia. His blood examination reveals basophilic stippling of RBCs and microcytic anemia. What is the likely diagnosis?
A 30-year-old patient presents with nausea, weakness, headache, impaired vision, and high anion gap metabolic acidosis. What is the most likely cause?
Practice by Chapter
General Principles of Toxicology
Practice Questions
Antidotes and Specific Therapies
Practice Questions
Drug Overdose Management
Practice Questions
Heavy Metal Poisoning
Practice Questions
Pesticide and Insecticide Poisoning
Practice Questions
Plant and Food Toxins
Practice Questions
Household Chemical Exposure
Practice Questions
Environmental Toxins
Practice Questions
Occupational Exposures
Practice Questions
Toxicological Screening and Diagnosis
Practice Questions
Extracorporeal Removal Techniques
Practice Questions
Poisoning Prevention Strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app