
Rheumatology and Immunology — MCQs

On this page
Which of the following conditions is most commonly associated with disease activity in Systemic Lupus Erythematosus (SLE)?
Bilateral hilar lymphadenopathy, along with non-caseating granulomas, is a characteristic feature of:
A 20-year-old female has an erythematous rash over her face, including both cheeks and the bridge of her nose, which is exacerbated by sunlight exposure when she is outdoors. In addition to the rash, she has experienced muscle and joint pain for several months. Although radiographs of the joints do not reveal any abnormalities, she has normal joint mobility without deformity. Which laboratory test finding is most characteristic of systemic lupus erythematosus (SLE)?
In ankylosing spondylitis, joint involvement is least in?
A person presents with recurrent swelling on the face and lips due to emotional stress. The likely cause is?
All of the following are true about Drug-Induced Lupus in comparison to Idiopathic SLE, except:
Which type of arthritis is commonly associated with tarsal tunnel syndrome?
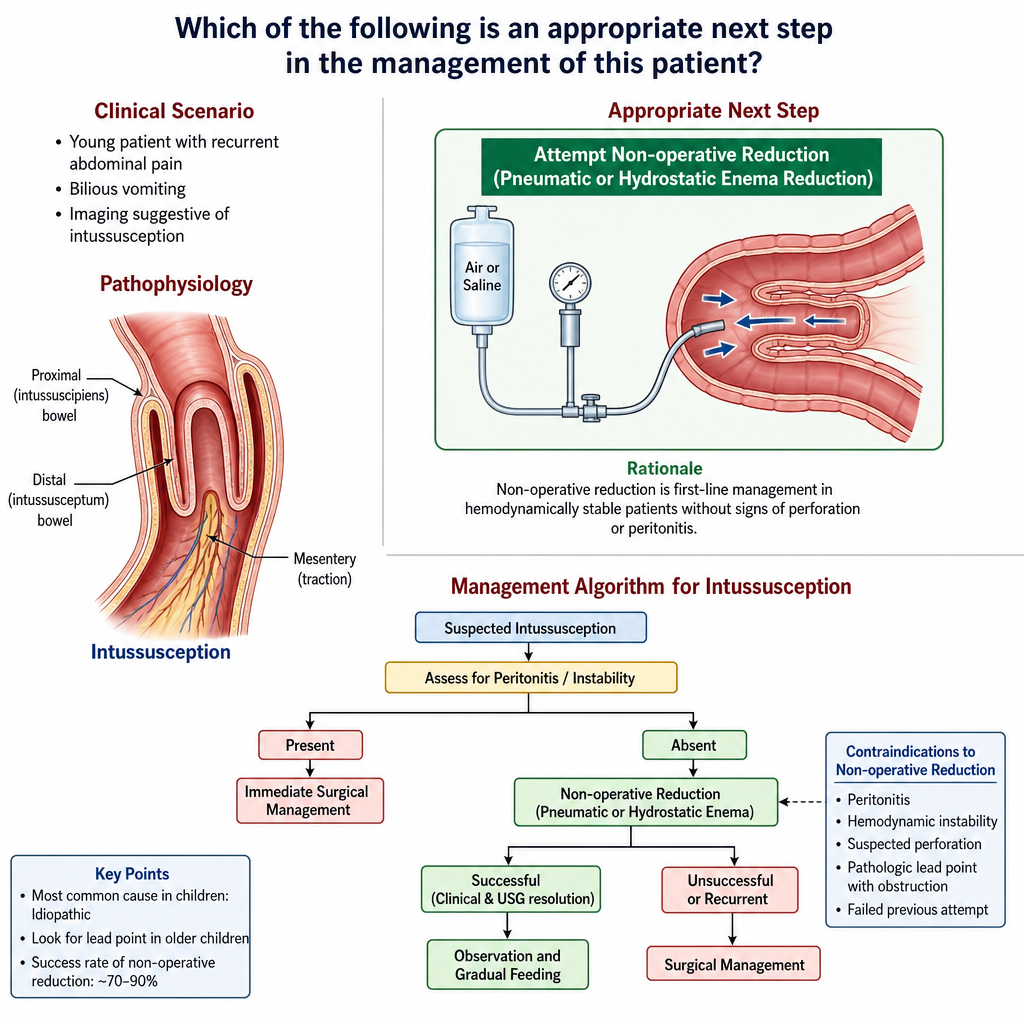
Which of the following is an appropriate next step in the management of this patient?
Normal CRP with elevated ESR is seen in:
A 35-year-old woman complains of aching all over, with symptoms that have progressed over several years, and reports pain and weakness causing her to drop things. Physical examination reveals multiple points of tenderness over the neck, shoulders, elbows, and wrists, with no joint swelling or deformity. Laboratory tests, including complete blood count and ESR, are normal, and rheumatoid factor is negative. Which is the best therapeutic option for this patient?
Practice by Chapter
Rheumatoid Arthritis
Practice Questions
Spondyloarthropathies
Practice Questions
Systemic Lupus Erythematosus
Practice Questions
Vasculitis Syndromes
Practice Questions
Scleroderma and Related Disorders
Practice Questions
Inflammatory Myopathies
Practice Questions
Crystal Arthropathies
Practice Questions
Osteoarthritis
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Autoinflammatory Syndromes
Practice Questions
Sjögren's Syndrome
Practice Questions
Antiphospholipid Syndrome
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app