
Rheumatology and Immunology — MCQs

On this page
Most common form of psoriatic arthritis
Which arthritis is commonly associated with uveitis?
Poly arteritis nodosa does not involve
The common HLA type associated with Behcet disease is _________
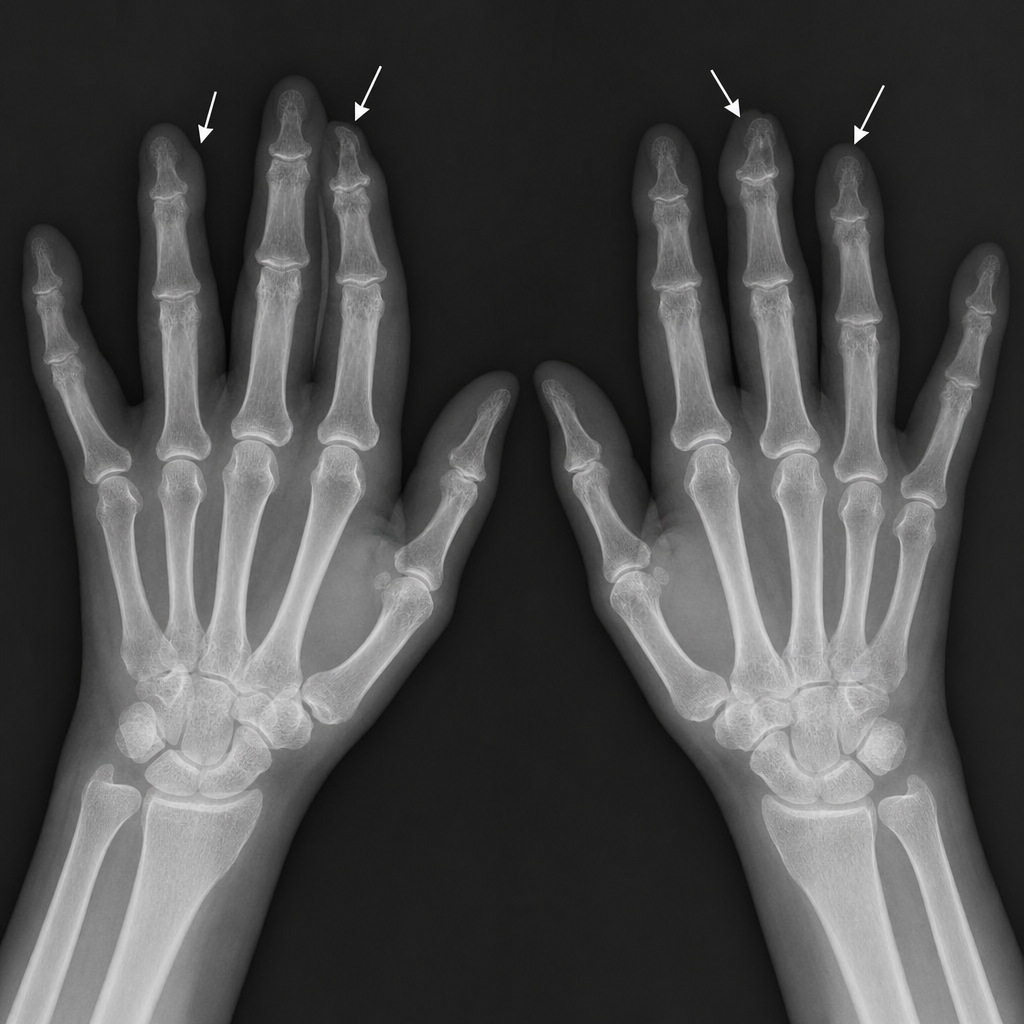
A 55-yrs-old woman complains of stiff, aching hands, especially in the morning. Radiographs of the hands reveal expansion at the base of the terminal phalanges & tapering of the proximal phalanges. This patient most likely has:
Vasanti, 28-year-old, presents with complaints of tightness of fingers. There is also history of dysphagia. Which of the following is the probable diagnosis:
Which of the following is true about rheumatic fever
All are true about gout except:
A 28-year-old woman with limited cutaneous scleroderma for the past 10 years complains of shortness of breath for the last month. What is the most likely diagnosis?
Following are listed as (SpA) spondyloarthritis features except
Practice by Chapter
Rheumatoid Arthritis
Practice Questions
Spondyloarthropathies
Practice Questions
Systemic Lupus Erythematosus
Practice Questions
Vasculitis Syndromes
Practice Questions
Scleroderma and Related Disorders
Practice Questions
Inflammatory Myopathies
Practice Questions
Crystal Arthropathies
Practice Questions
Osteoarthritis
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Autoinflammatory Syndromes
Practice Questions
Sjögren's Syndrome
Practice Questions
Antiphospholipid Syndrome
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app