
Rheumatology and Immunology — MCQs

On this page
True regarding felty's syndrome is all, except -
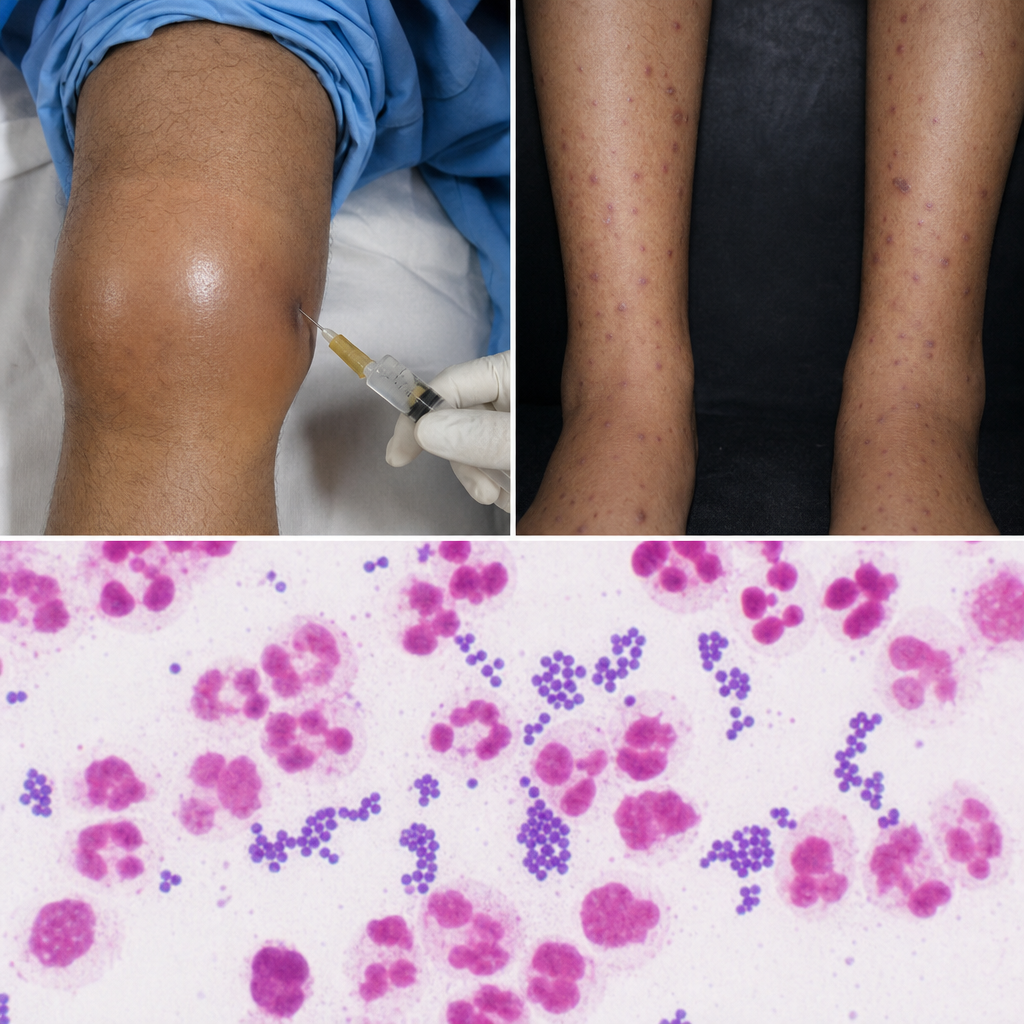
A 30-year-old male presented with fever with chills and migratory polyarthralgias. On examination some skin lesions were noted. Aspiration was done from the painful left knee and subjected to gram-staining, revealing intracellular gram-negative diplococci consistent with Neisseria gonorrhoeae. The patient reported of similar Neisseria infections in the past which led to frequent hospitalizations. Which of the following should be screened for in the above patient:-
All are true about Sjogren syndrome except
Which of the following is the least common site of pain in a case of rheumatoid arthritis?
All are true about Raynaud’s phenomena except:
Vigorous treatment of nephritis in SLE is indicated in:
All of the following conditions are observed in Gout except
Increased frequency of HLA-B 27 is seen in all the following diseases except
Behcet's disease is characterized by all of the following Except
A man takes peanut and develops tongue swelling, neck swelling, stridor, hoarseness of voice. What is the probable diagnosis?
Practice by Chapter
Rheumatoid Arthritis
Practice Questions
Spondyloarthropathies
Practice Questions
Systemic Lupus Erythematosus
Practice Questions
Vasculitis Syndromes
Practice Questions
Scleroderma and Related Disorders
Practice Questions
Inflammatory Myopathies
Practice Questions
Crystal Arthropathies
Practice Questions
Osteoarthritis
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Autoinflammatory Syndromes
Practice Questions
Sjögren's Syndrome
Practice Questions
Antiphospholipid Syndrome
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app