
Rheumatology and Immunology — MCQs

On this page
Which of the following are correct about Felty's syndrome? 1. It is associated with rheumatoid arthritis. 2. It may present with leukopenia. 3. It may have splenomegaly. 4. Splenectomy always improves the blood picture.
A patient presents with severe pain and swelling in his knee joint for 10 days. He also complains of pain and discomfort during urination. He says that he had diarrhea one month ago and he has been unwell since then. What is the most likely diagnosis?
A patient presents with pulmonary hemorrhage and is P-ANCA positive. What is the most likely diagnosis?
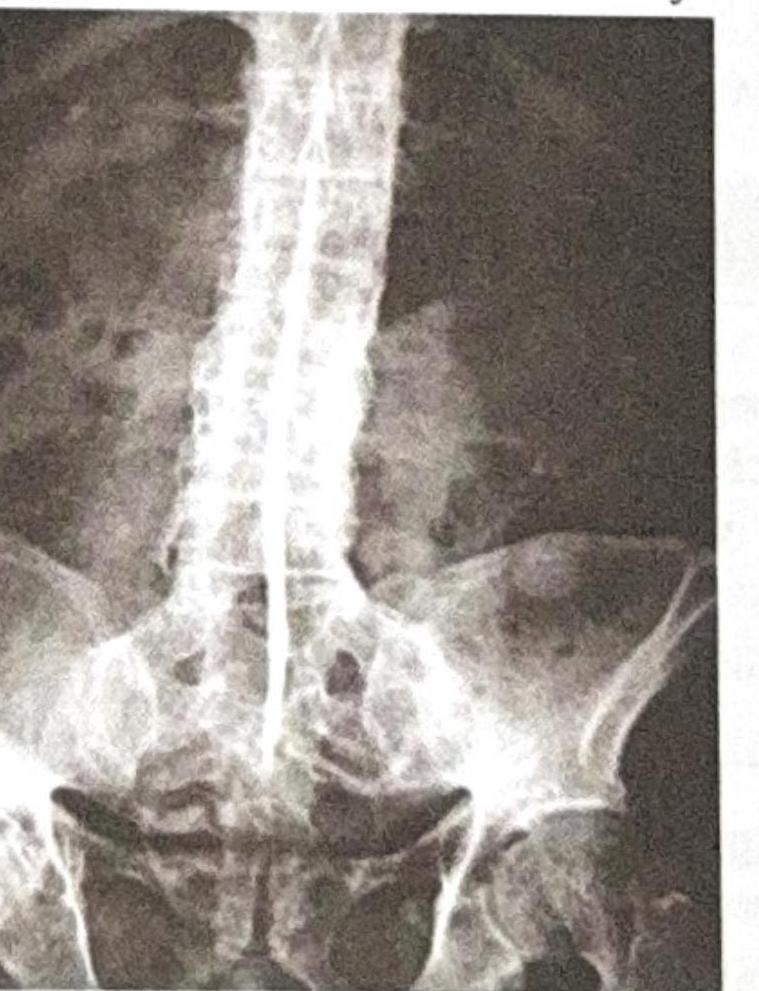
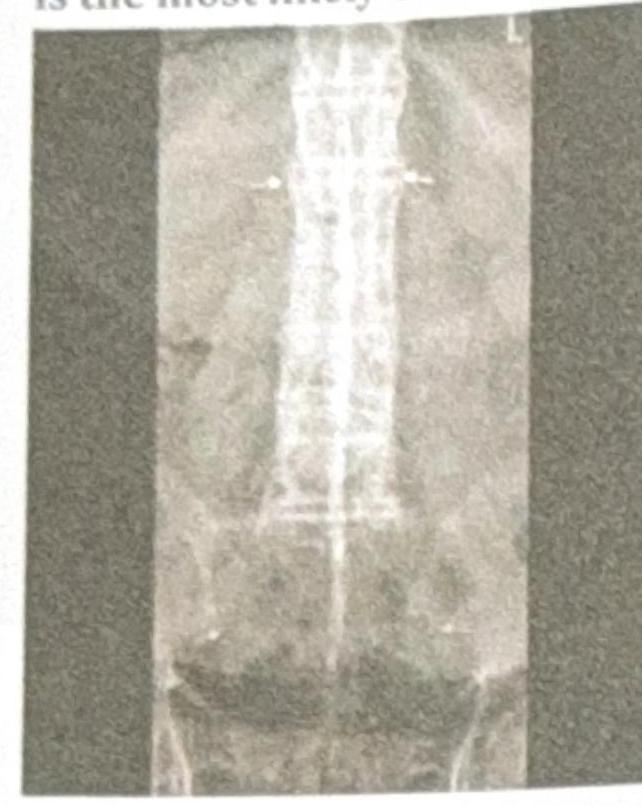
A 50-year-old male presents with backache, morning stiffness, red eye, and ankle swelling. Based on the X-ray provided, what is the most likely diagnosis?

A 20-year-old patient presents with chronic low backache and early morning stiffness for the last 2 years. For the past 6 months, they have also experienced bilateral heel pain. What is the most likely diagnosis?
A 26-year-old male presents with backache, morning stiffness, reduced chest expansion, and reddening of the eyes. The X-ray provided is shown below. What is the most likely diagnosis?
A patient presents with numb fingertips and tight facial skin. ANA is positive with an immunofluorescence nucleolar pattern. What is the most likely diagnosis?
A young male presents with acute redness of the eye. His X-ray of the spine is shown below. What is the most likely condition?
A young patient presents to the clinic with erythematous lesions over the exposed areas of the skin like hands, arms, chest, etc. she also complaints of arthralgia and breathlessness. Which among the following antibodies will be useful in diagnosing this condition?
Which of the following is not a first-line drug for the management of a patient with rheumatoid arthritis?
Practice by Chapter
Rheumatoid Arthritis
Practice Questions
Spondyloarthropathies
Practice Questions
Systemic Lupus Erythematosus
Practice Questions
Vasculitis Syndromes
Practice Questions
Scleroderma and Related Disorders
Practice Questions
Inflammatory Myopathies
Practice Questions
Crystal Arthropathies
Practice Questions
Osteoarthritis
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Autoinflammatory Syndromes
Practice Questions
Sjögren's Syndrome
Practice Questions
Antiphospholipid Syndrome
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app