
Rheumatology and Immunology — MCQs

On this page
A 35-year-old smoker with chronic sinusitis came for consultation due to an episode of hemoptysis. On examination his eyelids were puffy and urine microscopic examination shows presence of RBC casts. CT chest was performed. What is the diagnosis?

A 35-year-old construction worker with prolonged occupational exposure to respirable crystalline silica and pre-existing seropositive rheumatoid arthritis complains of progressive difficulty in breathing. Chest X-ray was performed. What is the diagnosis?

A 55-year-old female with rheumatoid arthritis presents with continuous pain and swelling of bilateral hand joints despite an adequate-duration trial of maximally tolerated methotrexate with confirmed adherence. What is the best treatment plan for this patient?

A patient presents with neck pain and rigidity which gets relieved after bathing in hot water and exercise. Cervical X-ray is shown below. What is your diagnosis?

A 25-year-old lady presents with inability to form a fist and marked stiffening of joints. Diagnosis is:
The best drug for maintenance therapy of Systemic Lupus Erythematosus (SLE) during pregnancy is :
Treatment of first choice in acute Gout is
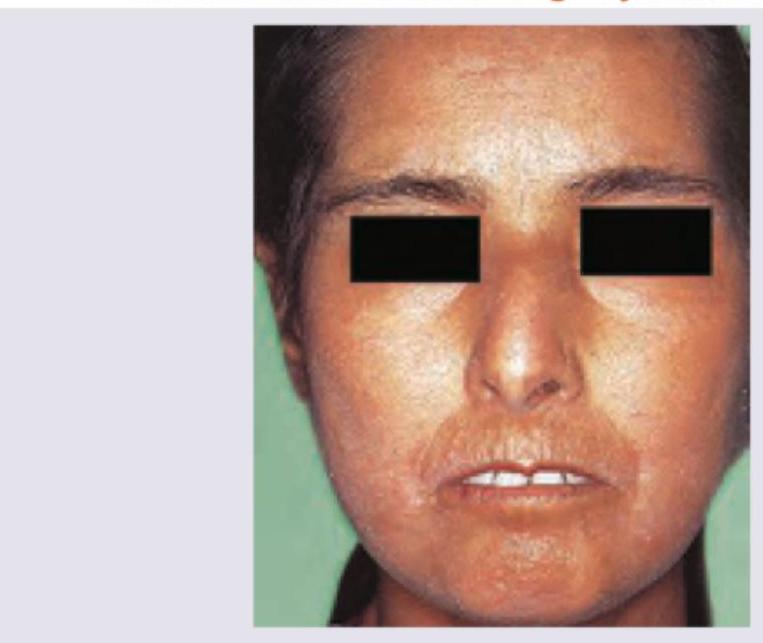
Which one of the following terms denotes the extensive sclerosis of the skin of the chest wall which restricts chest wall movement and is seen as a rare complication of systemic sclerosis?
Which one of the following statements is correct in respect of pulmonary involvement in rheumatoid disease?
A 40-year-old lady complains of progressive deformities of her hands and fingers associated with stiffness which is present in both the hands and improves as the day progresses. On examination, there is symmetrical involvement of hands and fingers of both the upper limbs with flexion and ulnar deviation at the metacarpophalangeal joints. What is the most likely diagnosis in this lady?
Practice by Chapter
Rheumatoid Arthritis
Practice Questions
Spondyloarthropathies
Practice Questions
Systemic Lupus Erythematosus
Practice Questions
Vasculitis Syndromes
Practice Questions
Scleroderma and Related Disorders
Practice Questions
Inflammatory Myopathies
Practice Questions
Crystal Arthropathies
Practice Questions
Osteoarthritis
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Autoinflammatory Syndromes
Practice Questions
Sjögren's Syndrome
Practice Questions
Antiphospholipid Syndrome
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app