
Rheumatology and Immunology — MCQs

On this page
A 40-year-old man presents with discomfort in one of his joints. Synovial fluid aspiration reveals rhomboid-shaped, positively birefringent crystals under polarized light microscopy. Which of the following is the most likely diagnosis?
Which of the following is the most common clinical feature observed during the progression of systemic lupus erythematosus (SLE)?
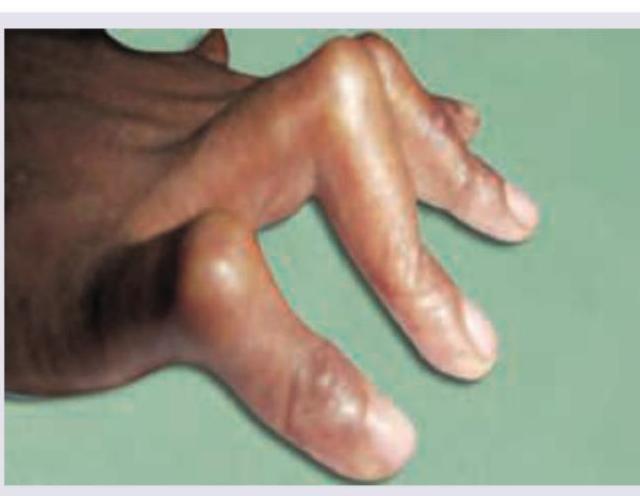
The deformity shown below is seen in:

A 30-year-old woman with Raynaud's phenomenon and difficulty in chewing food has the following physical appearance. Anti Scl-70 is positive. All are true about the condition shown except:

A 15-year-old girl has a persistent feverish feeling and myalgia. She has pain in the left knee joint and recurrent mouth ulcers. Which of the following tests is useful for diagnosis? (Recent NEET Pattern 2016-17)

A 25-year-old female presents with history of fever and oral ulcers and has developed erythematous lesions on her face. Comment on the diagnosis?

The clinical diagnosis favors development of chronic gout and the image shows presence of eccentric juxta-articular lobulated soft-tissue masses. Which of the following is the most definitive diagnostic test for gout shown in the image?

Identify the deformity shown in the image.
A 30-year-old female patient presents with erythematous rash over the neck, involving the back. Her investigations reveal presence of anti-MI-2 antibody. What is the diagnosis?

This elderly male came with a history of recurrent attacks of pain and swelling in the great toe in the past. This is the present X-ray of the hands. The diagnosis can be confirmed by:

Practice by Chapter
Rheumatoid Arthritis
Practice Questions
Spondyloarthropathies
Practice Questions
Systemic Lupus Erythematosus
Practice Questions
Vasculitis Syndromes
Practice Questions
Scleroderma and Related Disorders
Practice Questions
Inflammatory Myopathies
Practice Questions
Crystal Arthropathies
Practice Questions
Osteoarthritis
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Autoinflammatory Syndromes
Practice Questions
Sjögren's Syndrome
Practice Questions
Antiphospholipid Syndrome
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app