
Rheumatology and Immunology — MCQs

On this page
A young male develops serous otitis media of the left ear with cough, occasional hemoptysis, hematuria, and epistaxis for 2 months. His Hb is 7.5 g% with heavy proteinuria, BP 170/100 mmHg, RA negative, and ANCA positive. What is the most probable diagnosis?
Which disease characteristically involves the distal interphalangeal joint?
A patient complains of hematuria. Renal biopsy demonstrates a focal necrotizing glomerulonephritis with crescent formation. The patient also complains of decreased sensation in the hands and feet. What is the next best investigation to diagnose the condition?
All of the following are increased in rheumatoid arthritis, except?
During the winter months, a 65-year-old man presents with livedo reticularis and purple fingertips. Other symptoms include arthralgia and weakness. Renal impairment is present on laboratory testing. Which of the following is the most likely diagnosis?
Which of the following conditions does NOT typically cause bone erosion?
A 19-year-old man has a chronic papulosquamous skin disorder involving his knees and elbows. He now has dull low back pain and morning stiffness that lasts a few hours. On examination, forward flexion at the lumbar spine is reduced, but neck movements are normal. There is stress tenderness of both sacroiliac joints. Which of the following is the most likely diagnosis?
What is the Rh factor?
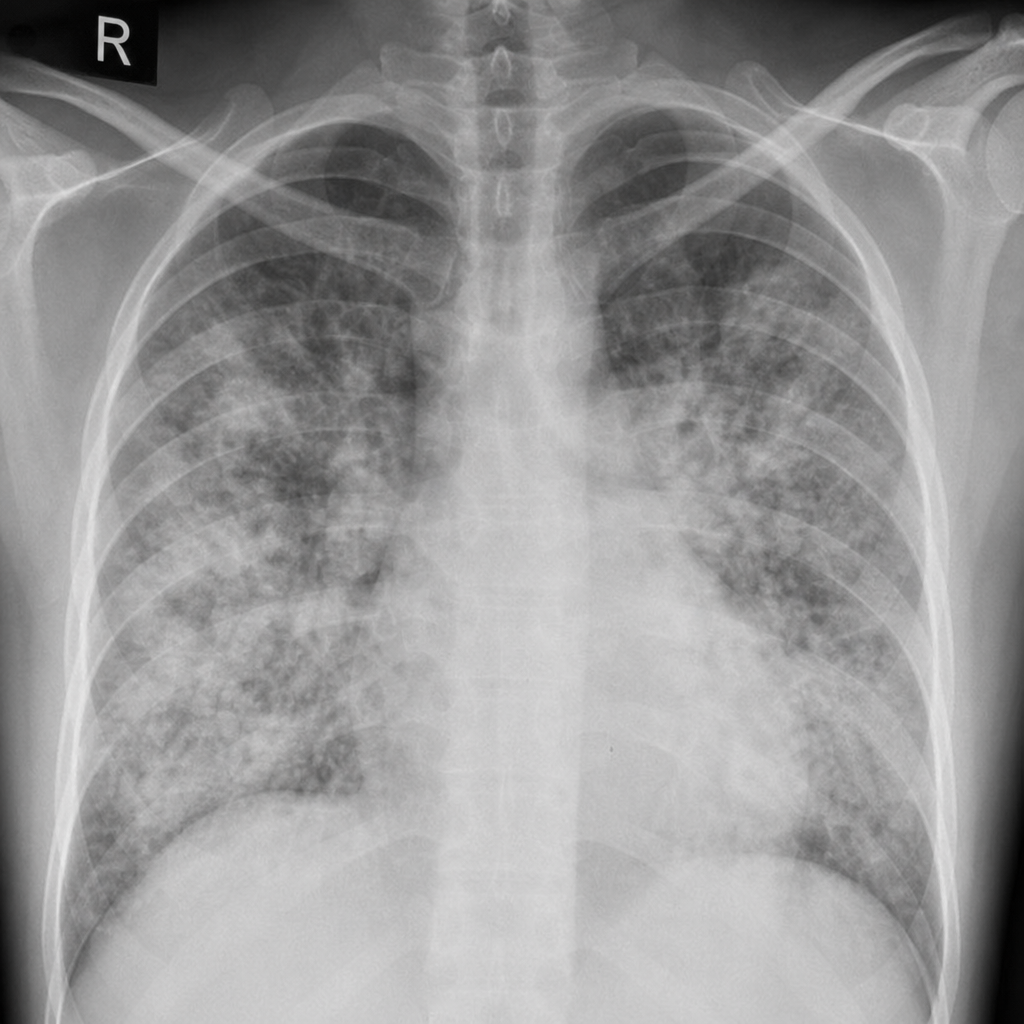
A 25-year-old normotensive patient presents to the emergency department with breathlessness and palpitations. The patient has a history of allergy to peanuts and accidentally ingested them. On examination, the patient has urticaria, diffuse wheezing, and bilateral crackles on auscultation. The heart rate is 120/min, blood pressure is 100/60 mm Hg, and SpO2 is 88% on room air. An urgent X-ray was performed and showed diffuse bilateral infiltrates without cardiomegaly. What is the most likely diagnosis?
This lesion is most commonly seen in which disease?

Practice by Chapter
Rheumatoid Arthritis
Practice Questions
Spondyloarthropathies
Practice Questions
Systemic Lupus Erythematosus
Practice Questions
Vasculitis Syndromes
Practice Questions
Scleroderma and Related Disorders
Practice Questions
Inflammatory Myopathies
Practice Questions
Crystal Arthropathies
Practice Questions
Osteoarthritis
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Autoinflammatory Syndromes
Practice Questions
Sjögren's Syndrome
Practice Questions
Antiphospholipid Syndrome
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app