
Rheumatology and Immunology — MCQs

On this page
Which of the following conditions is treated with this drug?

A 45-year-old male presented with severe pain in the knee and shoulder joints. A diagnosis of rheumatoid arthritis was made, and the patient was started on methotrexate 15mg weekly. However, after 6 months of methotrexate therapy, recurrent episodes of arthritis continued. The physician wants to add another DMARD that inhibits pyrimidine synthesis by inhibiting the dihydroorotate dehydrogenase enzyme. Which of the following drugs is the physician considering?
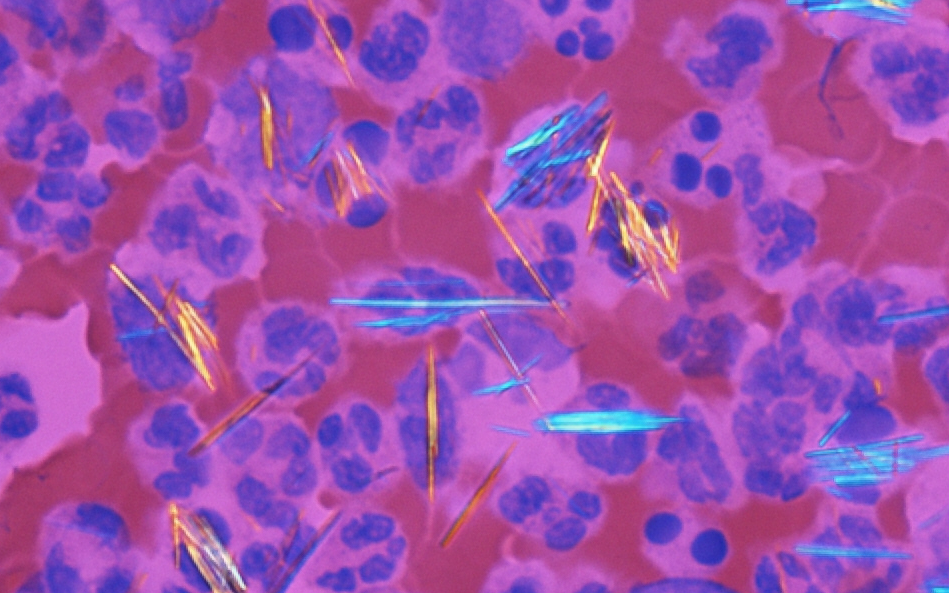
A 62-year-old male presented to the outpatient department with joint pain. He has experienced multiple gout flares over the past year and has no prior history of allopurinol intolerance or contraindication. The image shows findings from synovial fluid analysis. Which of the following drugs is used for the preferred first-line long-term urate-lowering therapy of this condition?
Which of the following is strongly associated with spondyloarthropathies?
All of the following statements about Antiphospholipid Antibody Syndrome (APLS) are true, EXCEPT:
All of the following are included in the Sydney revision of the Sapporo criteria for Antiphospholipid antibody syndrome EXCEPT:
Shrinking lung/kidney is seen in which of the following conditions?
A young female presents with diminished pulses in the upper limb and hypertension. What is the most likely diagnosis?
All of the following are true regarding Anti-phospholipid Syndrome EXCEPT:
Which of the following HLA antigens is associated with Sjögren's syndrome?
Practice by Chapter
Rheumatoid Arthritis
Practice Questions
Spondyloarthropathies
Practice Questions
Systemic Lupus Erythematosus
Practice Questions
Vasculitis Syndromes
Practice Questions
Scleroderma and Related Disorders
Practice Questions
Inflammatory Myopathies
Practice Questions
Crystal Arthropathies
Practice Questions
Osteoarthritis
Practice Questions
Primary Immunodeficiency Disorders
Practice Questions
Autoinflammatory Syndromes
Practice Questions
Sjögren's Syndrome
Practice Questions
Antiphospholipid Syndrome
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app