
Pulmonology — MCQs

On this page
Samters triad is seen in patients with ?
Upper lobe bronchiectasis is seen in which disease?
A male patient presents to the emergency department. The arterial blood gas report is as follows: pH, 7.2; pCO2, 81 mmHg; and HCO3, 40 meq/L. Which of the following is the most likely diagnosis?
A patient with a history of carcinoma of the bladder presents with dyspnoea, clinical signs of deep vein thrombosis (DVT), and tachycardia. Based on the Wells score for pulmonary embolism, what is the risk classification for this patient?
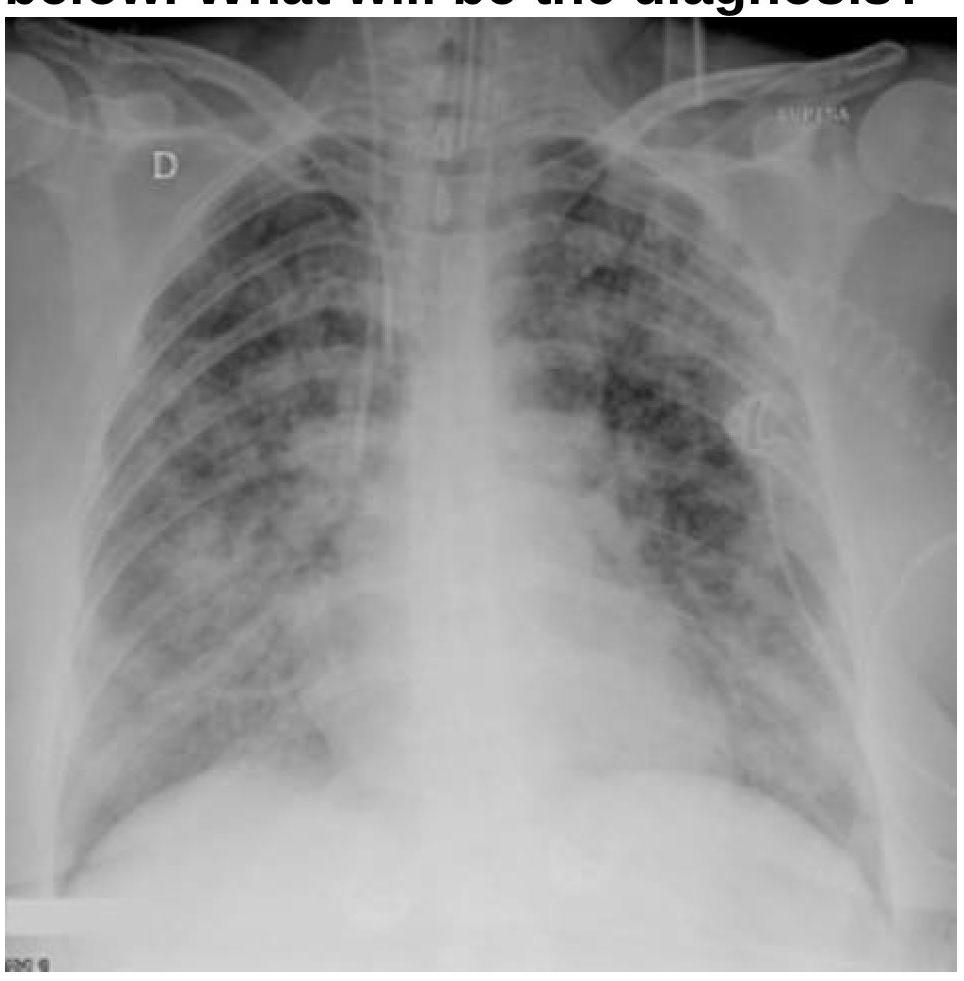
A patient with a known case of acute pancreatitis develops breathlessness and bilateral basal crepitations on day 4. What is the most likely diagnosis based on the chest radiography image?
Which of the following is least likely to be associated with allergic bronchopulmonary aspergillosis (ABPA)?
What does a decreased FEV1/FVC ratio typically indicate in pulmonary function tests?
Oxygen therapy may not be useful in
All of the following may lead to pneumatocele formation except which of the following?
Central bronchiectasis is seen with
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app