
Pulmonology — MCQs

On this page
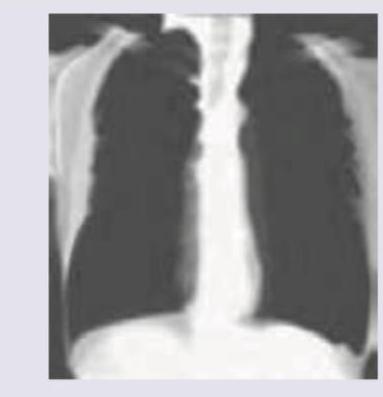
A 35-year-old coal worker presents with difficulty in breathing on exertion for last 2 years. CXR was performed. It shows:
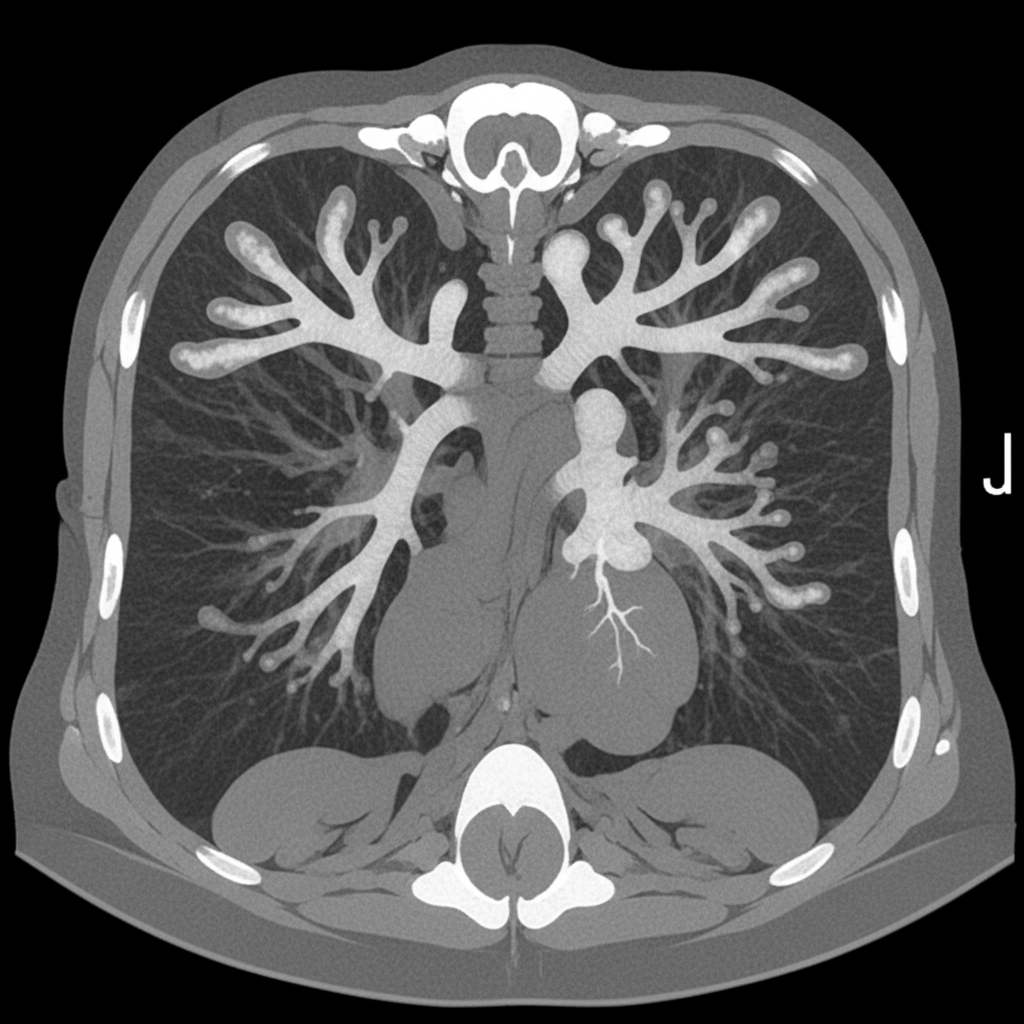
An asthmatic presents with brownish plugs in sputum. CT chest was performed. What is the diagnosis?
A 62-year old male chronic smoker has been diagnosed with Chronic Obstructive Pulmonary Disease (COPD). On pulmonary function testing, the ratio of Forced Expiratory Volume in 1 second (FEV1) to Forced Vital Capacity (FVC) was 0.6 and FEV1 was 70 % of predicted. What is the severity of airflow obstruction in this patient as per GOLD criteria?
Under the Stepwise Approach to the management of Bronchial Asthma, which one of the following is the correct initial treatment at Step 1 for a patient diagnosed with Asthma?
Consider the following statements: The clinical features of tension pneumothorax include 1. tracheal shift to contralateral side 2. absent breath sounds on the affected side 3. low output circulatory failure 4. peripheral cyanosis Which of the statements given above is/are correct?
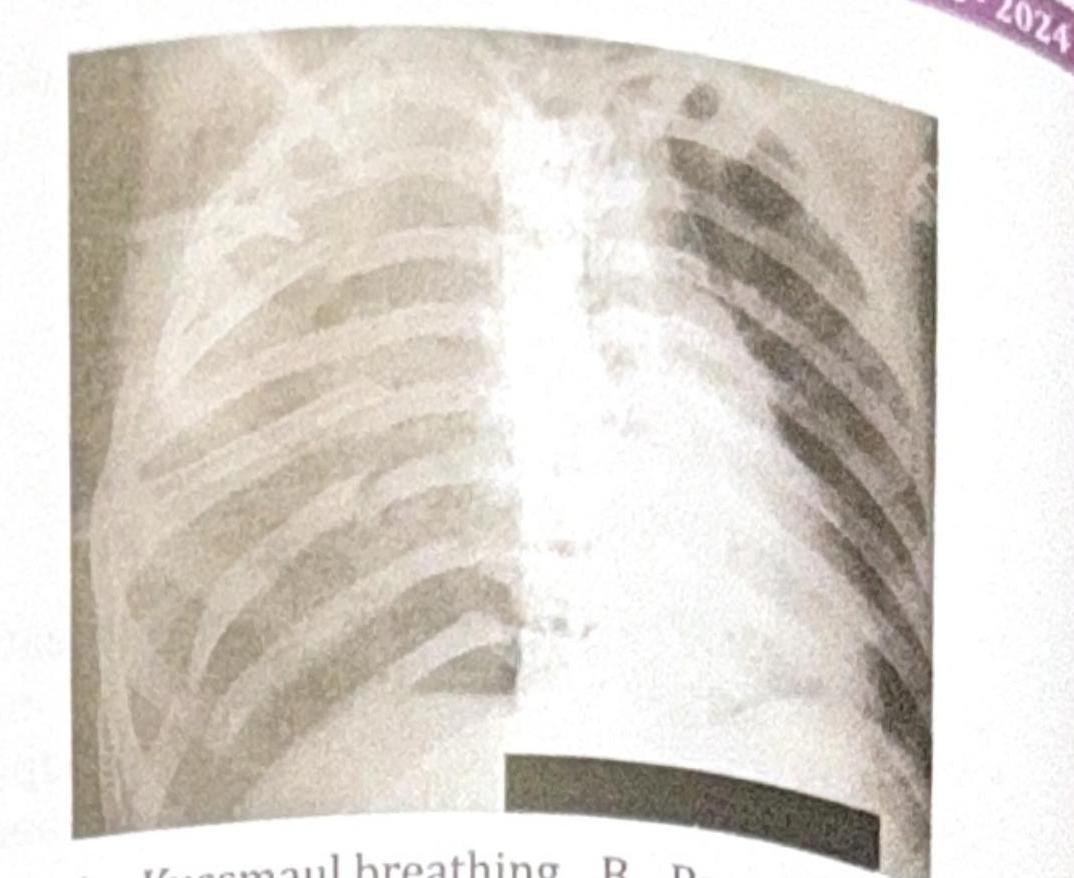
A 45-year-old male presents to the emergency department following a motor vehicle accident. He complains of severe chest pain and difficulty breathing. On examination, he appears distressed, with a respiratory rate of 28 breaths per minute. His oxygen saturation is 88% on room air. There is visible bruising on the chest, X-ray is done which is shown below. Which of the following is seen in this patient?
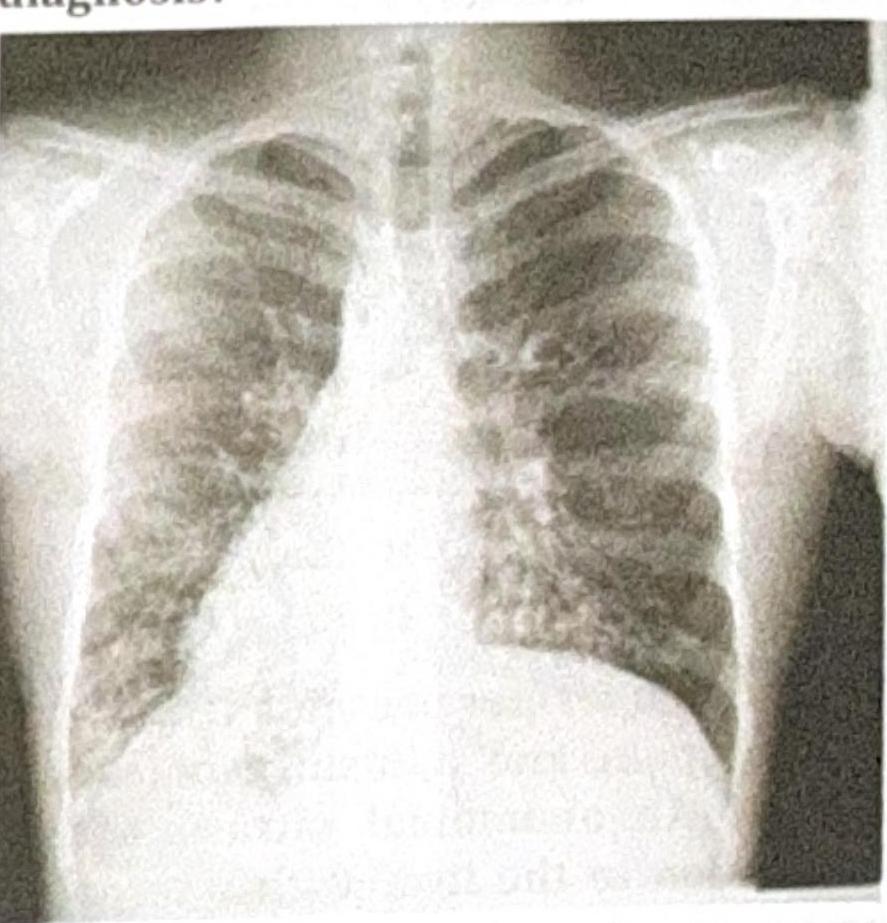
A 25-year-old patient presents with acute epigastric pain and elevated serum lipase. The patient was stabilized after 3 days, and a chest X-ray was obtained. What is the most common pulmonary complication associated with this condition?
A patient presents with respiratory distress and is diagnosed with panacinar emphysema. Which of the following is deficient?
A patient presents with recurrent lung infections, and the chest X-ray provided shows a characteristic finding. What is the most likely diagnosis?
Match the following: A) Caplan syndrome- 1) Found first in coal worker B) Asbestosis- 2) Upper lobe predominance C) Mesothelioma- 3) Involves lower lobe D) Sarcoidosis- 4) Pleural effusion is seen
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app