
Pulmonology — MCQs

On this page
A 35-year-old woman takes aspirin for a headache, later presented with wheezing and breathlessness. Along with these two symptoms, what other clinical findings are likely to be found in this condition?
A 58-year-old male with a 30-year smoking history presents with progressive dyspnea on exertion and dry cough for 8 months. Examination reveals bilateral fine inspiratory crackles at lung bases and digital clubbing. High-resolution CT chest shows bilateral subpleural reticular opacities with honeycombing predominantly in lower lobes. Pulmonary function tests show FEV1/FVC ratio of 0.85 with reduced DLCO. What is the most likely diagnosis?
A 45-year-old chronic smoker presents with complaints of dyspnea. Pulmonary function tests reveal FEV1/FVC ratio of 65% and RV/ TLC ratio of 141%. Which of the following best describes the underlying pathophysiology?
A patient with a known history of bronchial asthma is currently on salbutamol and ipratropium via MDI. He now presents with nocturnal worsening of symptoms and night time awakening. What is the next best step in management?
Patient with COPD presents with progressive dyspnea. ABG shows pH:7.32, pCO2 60 mm Hg and HCO3. which of the following is seen in
Old man underwent joint replacement surgery 3 days ago. Today he develops SOB with chest pain. O/E : pulse 100/min, BP 100/70 mm Hg, RR28/min and sp02: 85% room air. D-dimer is elevated. Which is the next best test
A patient is on salbutamol and ipratropium but continues to have nocturnal exacerbations of asthma. What is the next step?
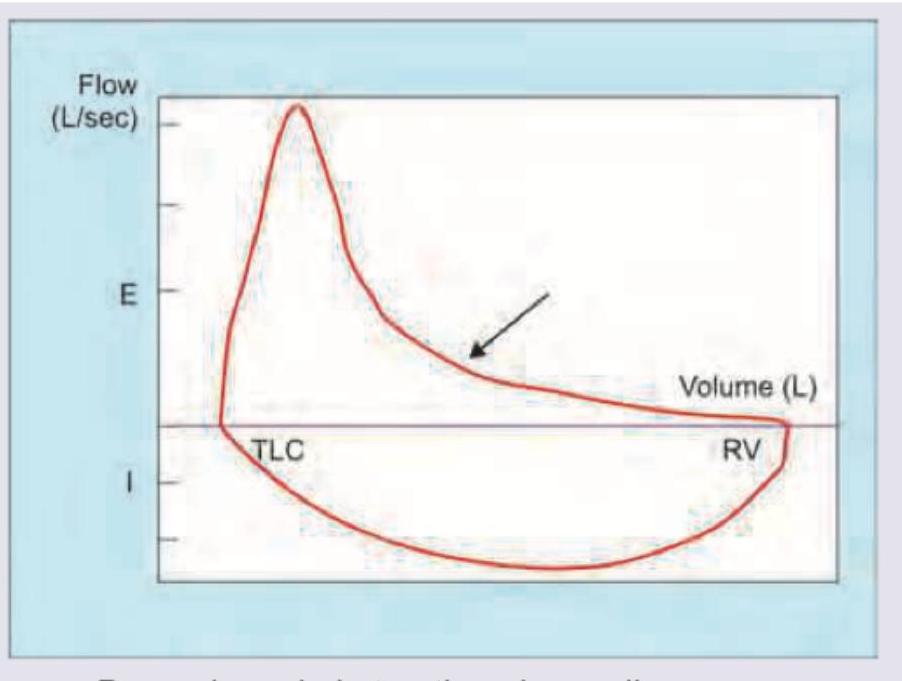
The following flow volume curve indicates:
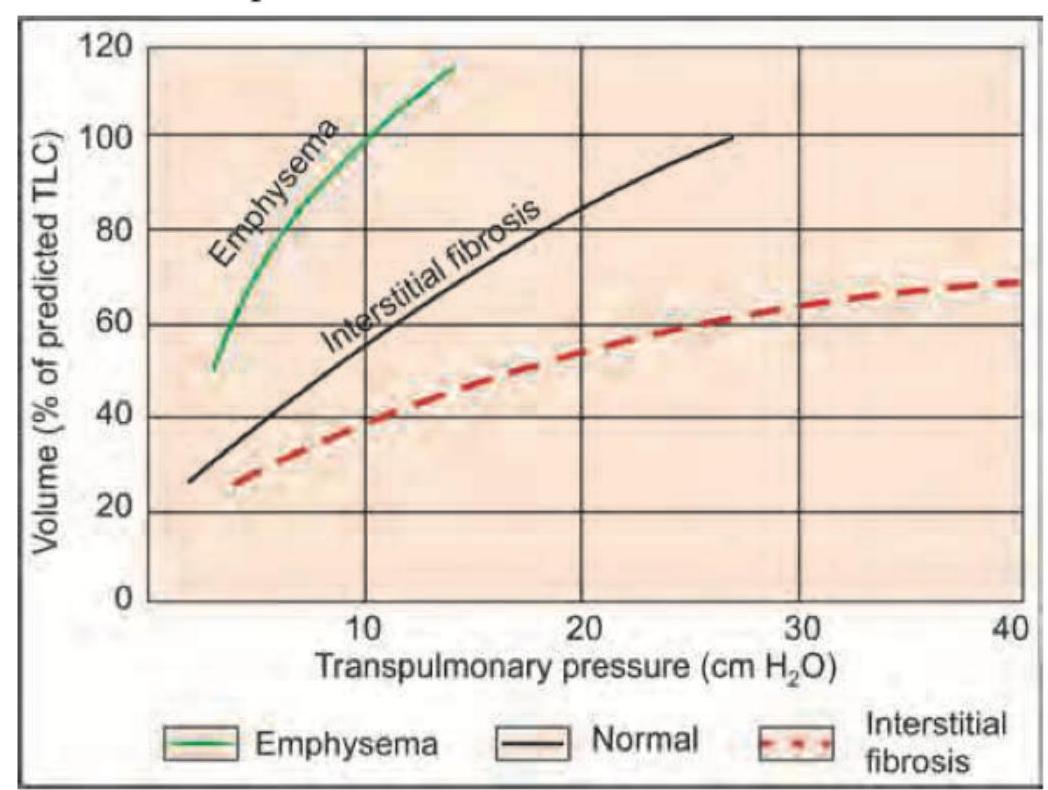
The curve shown is shifted downwards and to the right by which of the following?
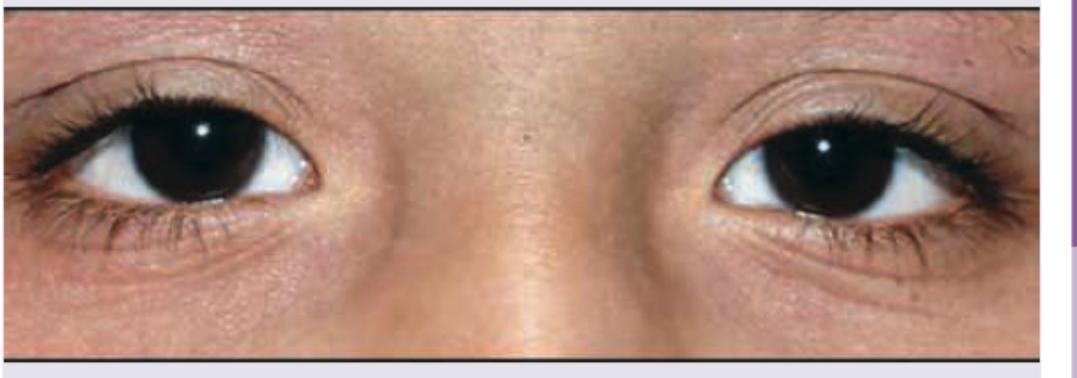
Which of the following is seen in the image?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app