
Pulmonology — MCQs

On this page
Which statement is true regarding pneumothorax?
Pulmonary embolism is most commonly caused by:
Which of the following statements about pulmonary embolism is false?
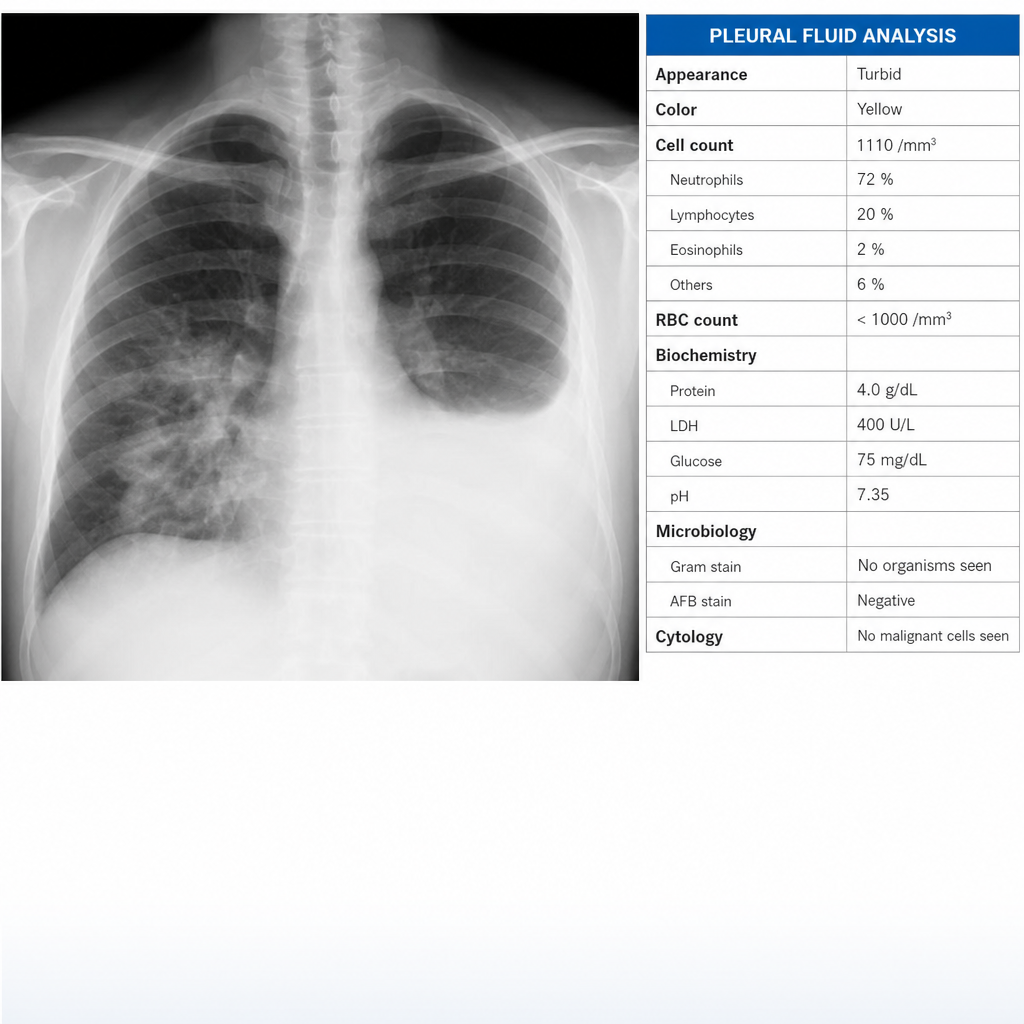
How should this pleural effusion be classified in a previously healthy 63-year-old man with pneumonia, as indicated by a chest x-ray showing consolidation and an ipsilateral pleural effusion, with pleural fluid analysis revealing a cell count of 1110/mm3 (neutrophil predominant), glucose of 75 mg/dL, protein of 4.0 g/dL, LDH of 400 U/L, pH of 7.35, and a negative Gram stain?
Hamman's sign is seen in:
Hemoptysis is said to be massive when it exceeds what amount in 24 hours?
Which of the following is the least likely cause of bronchiectasis?
Patient with pulmonary parenchymal fibrosis (PPF) who complains of breathing difficulty, is tachycardic, and tachypneic, and has a Batwing sign present on X-ray. What is the possible reason?

Most common clinical presentation of sarcoidosis is?
A 45-year-old man presents with a dry cough, fatigue, and bilateral hilar lymphadenopathy on chest X-ray. What is the most likely diagnosis?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app