
Pulmonology — MCQs

On this page
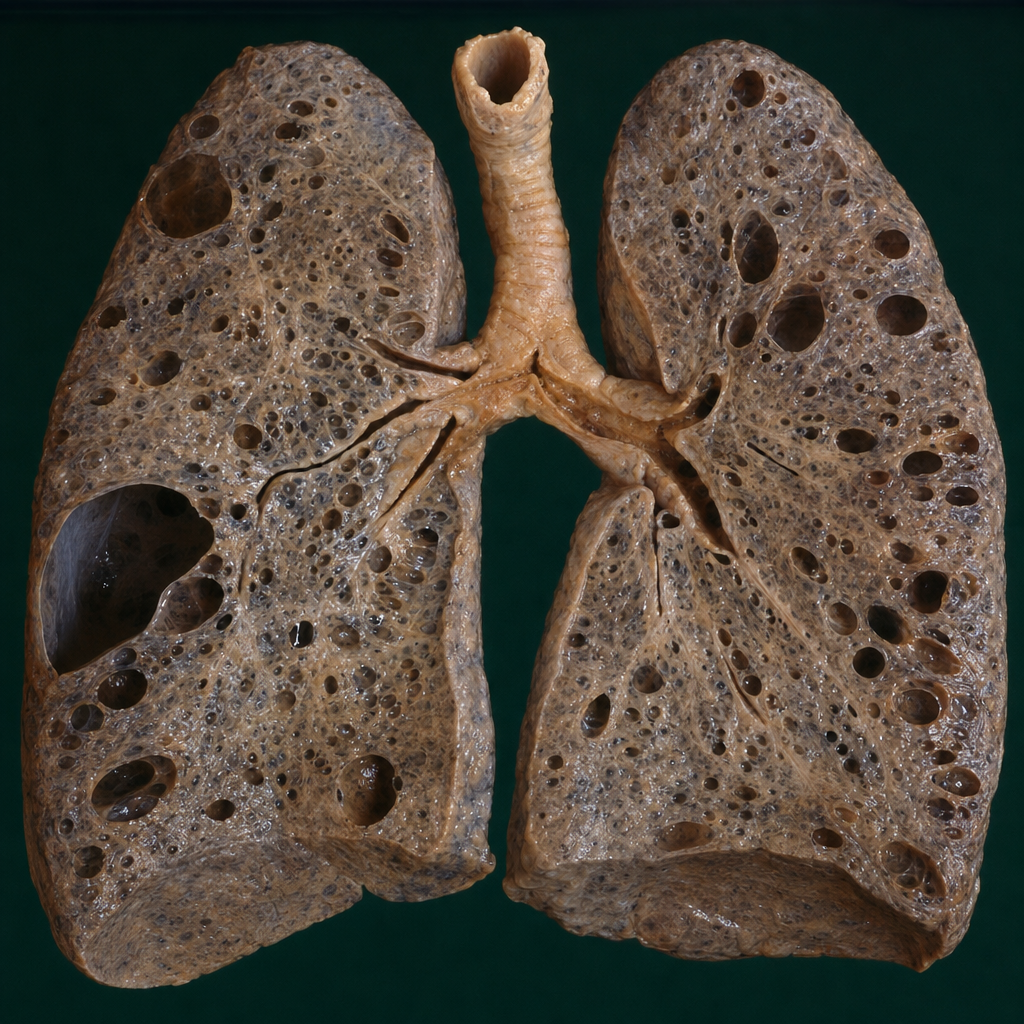
A 35-year-old woman with a long history of dyspnea, chronic cough, sputum production, and wheezing dies of respiratory failure following a bout of lobar pneumonia. She was not a smoker or an alcoholic. The lung autopsy is shown in the image. Which underlying condition is most likely associated with the pathologic changes shown?
A patient is a known case of acute pancreatitis who develops breathlessness and bilateral basal crepitations on day 4. What is the most likely diagnosis?
In which of the following conditions is oxygen therapy generally not considered useful?
A patient presents with symptoms of wheezing, shortness of breath, and a history of asthma. Which of the following conditions does this most likely signify?
Brock's syndrome is associated with which lobe of the lung?
Which tool objectively assesses the risk of adverse outcomes in a patient with pneumonia?
Type IV respiratory failure occurs due to
Which of the following lung conditions are smokers more prone to?
Lights criteria is used for
Which ECG pattern is commonly associated with pulmonary embolism?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app