
Pulmonology — MCQs

On this page
Which test is most useful for initial evaluation of suspected pulmonary sarcoidosis?
Which is the most common complication of deep vein thrombosis (DVT)?
Which test is most sensitive for screening/detecting pulmonary involvement in sarcoidosis?
A 50-year-old male presents with cyanosis and is diagnosed with chronic obstructive pulmonary disease (COPD). What is the primary mechanism causing his cyanosis?
A 55-year-old male with a history of bronchiectasis presents with acute onset of massive hemoptysis. What is the most appropriate immediate intervention?
A 55-year-old male presents with chronic cough and dyspnea. He has a 40-pack-year smoking history. His chest CT shows emphysematous changes. What is the most appropriate pharmacologic management?
Which of the following is the most common cause of hemoptysis in developed countries?
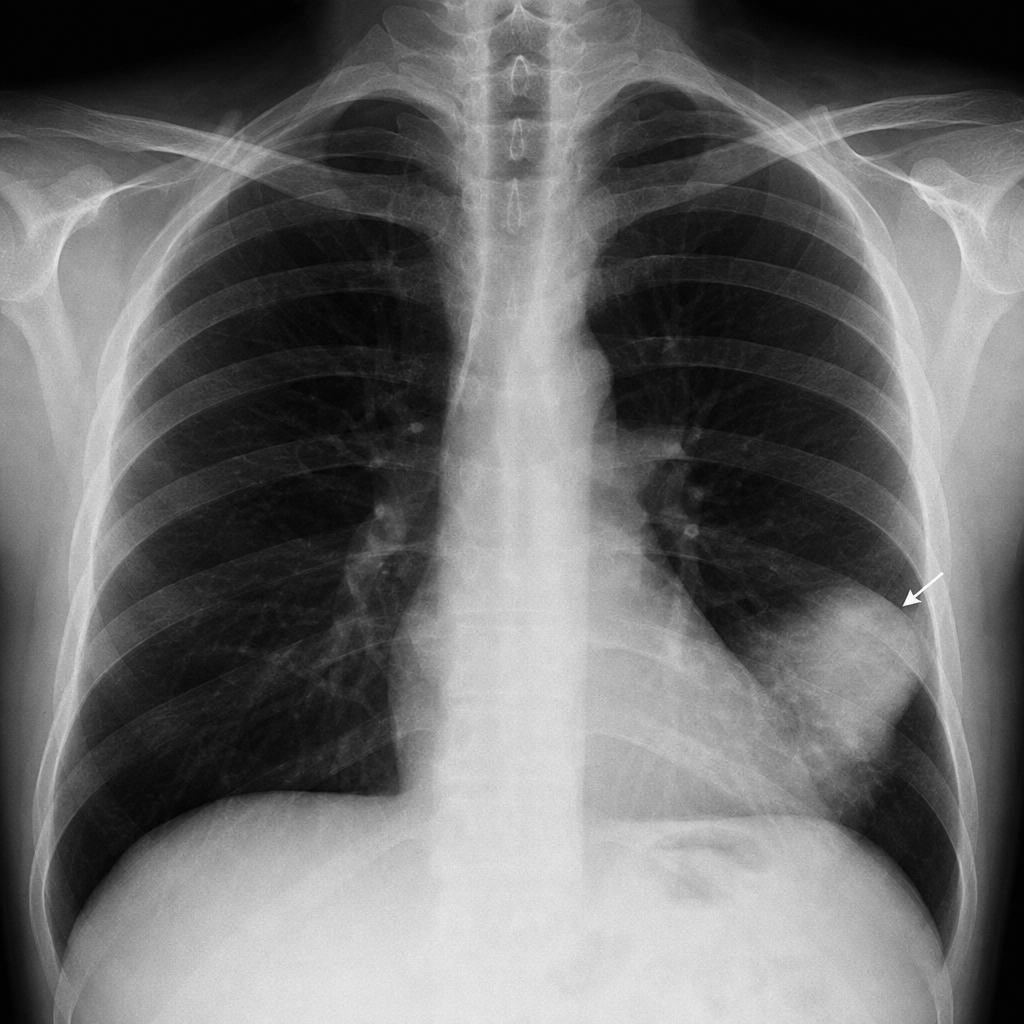
A 60-year-old male presents with sudden onset of pleuritic chest pain and dyspnea. Chest X-ray shows a wedge-shaped opacity in the lung. What is the most likely diagnosis?
All of the following can cause a chronic cough EXCEPT which of the following?
A patient with a history of chronic bronchitis presents with peripheral cyanosis and bilateral leg swelling. Which pathophysiological mechanism is most likely responsible?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app